
Back Herniated Disc Diagnosis & Treatment
Pain is a leading cause of work related back disability in people under the age of 45. Less than 15% will have an underlying nerve root problem related to a back herniated disc. The majority have a non-nerve back pain and most of these are assumed to be related to muscle or ligament injury or changes associated with disc degeneration. Despite this, little attempts are made to arrive at a specific diagnosis. Nonspecific diagnoses such as lumbar strain/sprain or lower back pain of unknown origin are very common.
Nerve pain related to a disc herniation is called radicular pain. Somatic pain is from a number of sources including muscles, joints and the disc itself. This can lead to confusion since pain patterns and symptoms may be similar. We will see if we can sort some of this out and make some sense of a pretty difficult situation.
Basic Disc Anatomy
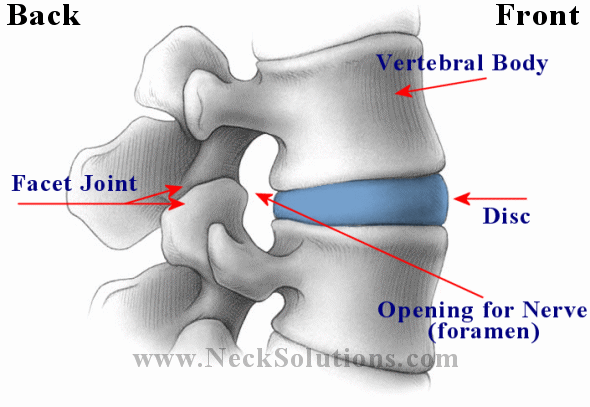
Lets take a look above at the basic anatomy of the disc and the vertebral unit. From the outside, you can see the disc, the top and bottom vertebrae (spinal bones) and the joints. The joints are the disc and its top and bottom vertebrae and the facet joints (2 on each side) in the back. While both joints are involved with motion, basically, the disc joint is involved in resisting compression, while the facet joints are involved with gliding. The back of the disc and the front of the facet joints form the foramen, which is an opening for the nerve that comes off the spinal cord.
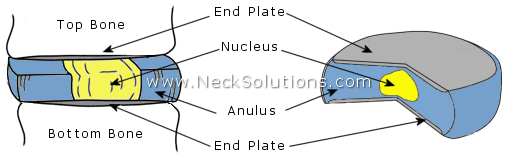
Taking it apart, you can see that the disc is made up of 2 parts; the annulus is the outer part in blue and the nucleus is the center part in yellow. You can also see the ends of the bones which go at the top and bottom of the disc have end plates, which are thin plates of cartilage.
What Happens In A Back Herniated Disc
A good analogy is comparing the disc to a jelly doughnut. The doughnut (annulus) and the jelly (nucleus). As we will see, the process of disc problems including herniations, are like the doughnut forming weak spots or tears from injury which allows the jelly to come out of place and push towards the outside of the doughnut. The jelly can bulge or protrude from the inside towards the outside or it can push all the way through the outside.

Looking from above down with the top vertebra (bone) removed, we can see a nice view of the disc and surrounding structures. The nerves come off the spinal cord, which runs down an opening called the spinal canal formed by the bones connecting together. The spinal cord continues up the spine and connects to the brain. As it it runs down the spine, spinal nerves come off at each level, forming a connection between the brain and every part of the body.
 To the left we see a herniated disc putting pressure on the nerve. Here, the nucleus (jelly) is pushing the annulus (doughnut) and the disc is herniated, protruding or bulging out enough to place significant pressure on the nerve root.
To the left we see a herniated disc putting pressure on the nerve. Here, the nucleus (jelly) is pushing the annulus (doughnut) and the disc is herniated, protruding or bulging out enough to place significant pressure on the nerve root.
This causes not only back pain, but pain, numbness and tingling (paresthesia) in the area that the nerve runs to, often referred to as radiculitis. It can be in the hip region, into the thigh, leg and even into the foot. We will see the general patterns that a herniated disc in the lower back causes for different levels of nerve pressure or pinching.
This can happen as a gradual process or all at once and can cause pain ranging from irritating to severe. Pain from a herniated disc referred down the leg is referred to as sciatica. There can be inflammation and muscle spasm as the muscles tighten to protect the sensitive nerves, often called muscle guarding.
 Traction & Inversion
Traction & Inversion Supports & Cushions
Supports & Cushions Belts & Corsets
Belts & CorsetsWe had mentioned the disc mainly resists compression forces, so the pain will be worse when there is more pressure on the disc. There can be pain when coughing, sneezing or straining. The pain will be worse when sitting, somewhat better when standing and not as bad when lying down. If you are holding an object, the pain will be worse the further out from the body and will be better the closer you hold it to your body – this is simple physics. Also, since the disc absorbs water, when you sleep at night, the pressure inside the disc is the greatest. Therefore, you should not do any heavy lifting when you first get out of bed as you are most likely to herniate a disc when the pressure is the greatest.
Types Of Back Herniated Disc
Terms used when describing disc herniations are often confusing. There is no simple way out of this. Different radiologists will use different terms depending on the sources of the information. A disc can be described as bulging, protruding, herniated, ruptured, prolapsed, extruded or sequestered; and further detailed regarding shape such as focal, localized or diffuse, generalized; or location as in central, medial (to the inside) or lateral (to the outside) of the nerve.
Symptoms may vary differ depending on these variables. A “slipped disc” is not a technical term and provides no information. There can be an intravertebral herniation called a Schmorl’s node where there is a break in the vertebral body endplate. Some use terms related to the ligaments, like sub-ligamentous.
In general, the disc herniation is noted as contained – the nucleus within the contents of the annulus (jelly inside of doughnut) or non-contained – the nucleus outside the contents of the annulus (jelly outside the doughnut).

The above illustrates types of back herniated disc. You may agree or disagree and, in general, you are right either way. Again, it depends on the source used. Some consider a herniation to be a specific type of disc displacement. So, there is no uniform description of disc herniation that is used by everyone. Additionally, the symptoms vary; there may be a disc bulge with no pain and there may be a disc bulge that produces a lot of pain. Smaller, painful disc herniations may be more difficult to treat than larger, extruded herniations.
Migrated or sequestered fragments from a disc herniation in the covering of the spinal cord (dura) can cause persistent low back pain symptoms. Missed, migrated disc fragments can be a cause of low back pain, radiculopathy or cauda equina syndrome, especially even in the absence of visible disc herniation. Suspicion needs to be maintained with unexplained and persistent symptoms with no obvious disc herniation on MR images.[1]
A finding on MRI called Modic changes are associate with back pain. Specifically, Modic Type 1 changes are associated with a poorly healing back herniated disc and are, in some cases, indicative of a low grade bacterial infection, which have responded to antibiotics for relief of back pain.
Internal Disc Disruption & High Intensity Zone
 One commonly overlooked source of chronic low back pain is internal disruption of the intervertebral disc. A disc can cause back and leg pain without involving the nerve root. This is disc mediated somatic pain as the disc is a potential pain generator.
One commonly overlooked source of chronic low back pain is internal disruption of the intervertebral disc. A disc can cause back and leg pain without involving the nerve root. This is disc mediated somatic pain as the disc is a potential pain generator.
Internal disc disruption shows a loss of normal distinction between the nucleus and the annulus, disorganization and fissuring (tearing) of the annulus, a preserved external disc contour and appearance and absence of nerve root compression. The disc appears externally intact and undeformed on imaging but revealed painful annular pathology on discography.
Internal disc disruption is common; nearly 30% to 50% of those with chronic low back pain have internal disc disruption. A clinical diagnosis of internal disc disruption based on history and physical examination alone is extremely difficult. Most of the patients experience diffuse, dull ache or a deep seated, burning, lancinating pain in the back. Some will complain of a sensation of a weak, unstable back. Referral of pain into the hips and lower limbs is not uncommon.
 Massage Tools
Massage Tools Relief Supplements
Relief Supplements Topical Relievers
Topical RelieversTears in the annulus part of the disc, indicated on MRI by a high intensity zone (HIZ), cause high levels of inflammation responsible for back pain. A disc with moderate levels of degeneration and a high intensity zone is diagnostic of a painful herniated disc.[2]A high intensity zone on MRI located in the back (posterior) and bottom (inferior) part of the annulus is common indication of disc disruption and significant when diagnosing back pain related to the disc (discogenic back pain).[3]
 A high intensity zone is a risk factor for recurring low back pain, almost twice as likely to suffer another pain episode. Higher levels of degeneration to be predicative of a future back pain occurrence. The hazard for a future episode of back pain increases for each previous episode, noting the importance of MRI findings in predicting future risks of lower back pain episodes.[4]
A high intensity zone is a risk factor for recurring low back pain, almost twice as likely to suffer another pain episode. Higher levels of degeneration to be predicative of a future back pain occurrence. The hazard for a future episode of back pain increases for each previous episode, noting the importance of MRI findings in predicting future risks of lower back pain episodes.[4]
Individuals with severe acute back pain, without radiating pain or sciatica called axial back pain are significantly more likely to have a high intensity zone on MRI.[5] High intensity zones are a reliable indicator of painful disc disruption of the annulus.[6] They are relevant imaging biomarkers and are significantly associated with prolonged and severe low back pain as well as sciatica.[7]
Internal disc disruption is a common cause of disabling low back pain in a substantial number of young, healthy adults and repeated injury during active healing leads to persistent inflammation and enhanced disc degeneration.
High intensity zones are also associated with the presence of both Modic changes and end plate changes in the same motion segment, which the smallest section of the spine that can move as a single unit.[8]
Modic Changes
A back herniated disc will typically heal and resorb in time, however, if the herniation pulls a piece of the endplate with it, healing can be complicated. The endplate is a vital part of maintaining disc integrity. Damage can lead to painful conditions and allow bacteria to enter the disc and subsequent Modic changes due to a low grade infection, which complicates recovery with high levels of inflammation. Modic changes are associated with poor outcomes for herniated discs that become a chronic issue. This has been an overlooked source of chronic and disabling back pain.
Failure of the endplate junction is a common source of disc herniation. This break in the endplate not only allows for hernited disc material to extrude, but also provides a pathway for bacteria to enter, potentially causing infection associated with Modic changes. Endplate herniations contain cartilage and even pieces of bone and can complicate the recovery from a herniated disc.[9]
End plate damage causes decompression of the disc, disc height loss, which can result by cartilage being pulled from the bone attachment. This can cause disruption of the balance mechanism leading to degenerative changes and pose a risk factor for further damage.[10]
Disruption of the endplate can be fracturing or herniation and may relate to Modic changes (lesion to the endplate and bone marrow) that is frequently associated with inflammation, especially type 1. Pulling off of the endplate may lead to the erosion often seen at lower lumbar spine levels that are associated with pain and degeneration. Pulling off of cartilage and the underlying bone can happen with acute (sudden) or repetitive (gradual) disc herniation, and pose a risk to healing through absorption.
An endplate microfracture injury can induce Modic changes, disc degeneration and spinal cord sensitization.[11] Modic changes are a strong factor, especially for the young, for recurrent lumbar disc herniation 1 year after discectomy and reflect a reactive vertebral modification related to disc inflammation and an unstable microenvironment.[12]
Endplate changes on MRI are associated with degeneration, inflammation and nerve infiltration in herniated discs. Cartilage in the disc modulates degeneration and inflammation and indicates slow healing and persistent clinical symptoms.[13]
The level of inflammation in the disc is associated with the intensity of pain and disability. There is a direct correlation between separation of endplate cartilage and increased severity of disc herniation. The connection with endplate cartilage is an initial link in the mechanical failure of the intervertebral discs.[14]
Signs Of Disc Related Back Pain
The above findings of high intensity zones and Modic changes are good indicators that the pain is disc related. These are often found in chronic cases on MRI. If these are missed, patients can be told it just in their head or just a normal part of the aging process. Specific pain generator indications can lead to additional or other methods of treatment. So, even with a herniated disc, some complicating findings can be missed. It may also be that a herniated disc is not the main source of pain.
Reliable indicators of back pain due to disc problems may not present clinically as a typical disc herniation, but are related to disc damage, pain, and prolonged healing. These findings are High Intensity Zones and Modic changes, as discussed above. However, lets re-visit this for a moment, so it is clear and concise.
A High Intensity Zone (HIZ) seen on MRI is significant when seen in the posterior or back of the disc. It is fluid/mucoid material with new blood vessels and granulation tissue encased between torn fibers of disc annulus or under the posterior longitudinal ligament that runs along the back of the discs. They result mainly from mechanical loading fatigue, as well as inflammation due to repair of a disc tear.
Now a disc tear represents not only mechanical injury and inflammation, there is also a means for bacteria to enter in this special non-aerobic environment, thus providing conditions for a low grade bacterial infection as seen with some Modic changes. “So we conclude that HIZ on T2-weighted MR images is credible to forecast the discogenic LBP.”
Modic changes show as signal abnormalities on MRI in the bone marrow of the associated disc. These lesions of the endplates are confirmed to be associated with back pain from the disc. Modic changes are an accelerated form of disc degeneration that can go into the nucleus of the disc, beyond the annulus or outer part. Modic changes show a high diagnostic significance for disc related (discogenic) low back pain. “The results conducted by our research confirmed the association between the discogenic LBP and Modic change.”[15]
 New Mattresses
New Mattresses Heat Therapy
Heat Therapy Cold Therapy
Cold Therapy5 questions are useful in diagnosing disc related low back pain related to degeneration. A positive response of pain to 3 – 5 of the questions is indicative of degeneration related discogenic pain:[16]
- After sitting too long
- While standing after sitting too long
- Squirming in a chair after sitting too long
- While washing one’s face
- In the standing position with flexion (bending forward)
Disc pain is usually felt in the lumbar spine region and may be felt in the buttocks, down to the upper thighs. Radicular pain or pinching of the nerve usually presents with muscular weakness and sensory problems in the distribution of the buttock, lower abdomen, groin region, and lower extremities. There can be both involved.[17]
Findings Of A Back Herniated Disc
The assessment is based on history and physical examination which includes neurological examination, motor examination, sensory examination, reflex examination, and application of provocative maneuvers or orthopedic tests. This represents a more classic or textbook example of a herniated disc.
| Disc Herniation | L3-L4 | L4-L5 | L5-S1 |
| Nerve Root | L4 | L5 | S1 |
| Pain |  |
 |
 |
| Low back, hip, front/side thigh, inside leg | Above SI joint, hip, side thigh and leg, top of foot | Above SI joint, hip, back side thigh and leg, heel | |
| Numbness |  |
 |
 |
| Front inside thigh and knee | Side leg, first 3 toes | Back calf, side leg, heel and toe | |
| Atrophy – wasting | Quadriceps | Minor | Gastocnemius, soleus |
| Motor weakness | Extension of quadriceps | Dorsiflexion (pull up) great toe and foot (foot drop) | Plantar flexion (push down) great toe and foot |
| Screening exam | Squat and rise | Heel walking | Walking on toes |
| Reflexes | Knee jerk diminished | None | Ankle jerk diminished |
Sometimes, there will be a position that will make the pain worse or better, depending on the location of the herniated disc. Below is graphic which shows how a disc herniated medial (inside the nerve root) or lateral (outside the nerve root) can cause a person to assume a certain position called an antalgic lean.
As you can see, by examining which way a person with sciatica from a herniated disc leans, you can get an indication where the herniated disc is in relation to the nerve root.
Radiation of pain needs to be carefully interpreted. Somatic referred pain in the buttock or lower limb can be expected. Somatic referred pain is mostly in the buttock or lower extremity without any type of pain generators in the back and it should not be confused with radicular pain from a nerve root. The differences are in the quality of pain and its behavior. Below you can see the differences between radicular pain from a back herniated disc and somatic pain.
| Somatic or Referred Pain | Radicular Pain | |
| Segment Causes | Posterior segment or element | Anterior segment |
| Facet joint pain | Disc herniation | |
| Sacroiliac joint pain | Annular tear, discogenic pain | |
| Myofascial syndrome | Spinal stenosis | |
| Internal disc disruption | ||
| Symptoms | ||
| Dull, aching, deep | Sharp, shooting, superficial, lancinating | |
| Like an expanding pressure | Like an electric shock | |
| Poorly localized | Well localized | |
| Covers a wide area | Leg worse than back | |
| Back worse than leg | Paresthesia present | |
| No paresthesia | Well defined | |
| No radicular or shooting pain | Radicular distribution | |
| Modification | Worse with extension | Worse with flexion |
| Better with flexion | Better with extension | |
| No radicular pattern | Radicular pattern | |
| Radiation | Low back to hip, thigh, groin | Follows nerve distribution |
| Radiation below knee unusual | Radiation below knee common | |
| Quasi segmental | Radicular pattern | |
| Signs | ||
| Sensory Alteration | Uncommon | Probable |
| Motor Changes | Only subjective weakness | Objective weakness |
| Atrophy rare | Atrophy possibly present | |
| Reflex Changes | None | Commonly described, but seen only occasionally |
| Straight Leg Raises | Only low back pain | Reproduction of leg pain |
| No root tension signs | Positive root tension signs | |
| Adapted and modified from: Manchikanti L, et al. Low back and lumbar radicular pain. In: Manchikanti L, et al (eds). Clinical Aspects of Pain Medicine and Interventional Pain Management: A Comprehensive Review. ASIPP Publishing, Paducah, KY, 2011, pp 87-114 (374). | ||
Chronic, persistent low back, lower extremity pain, and radicular pain may be secondary to a back herniated disc, disc disruption, disc degeneration, spinal stenosis, or after surgery resulting in disc related pain with or without radiculitis. There is much information regarding cause, diagnosis, and numerous treatment methods for herniated disc pain. As we have noted, magnetic resonance imaging (MRI) findings of a herniated disc are not always accompanied by symptoms.
In individuals aged 25 to 55 years, about 95% of herniated discs occur in the low back called the lumbar spine at the L4/5 and L5/S1 levels more common in men; disc herniation above this level is more common in people aged over 55 years and upper lumbar disc herniation may be associated with hip pain and/or groin pain. Disc displacement may present as internal disc disruption, disc prolapse, disc protrusion, disc extrusion, disc herniation, or simply discogenic pain.
A thoracic disc herniation (mid/upper back) can result in pain, sensory disturbances, myelopathy, and lower extremity weakness. There may be extraspinal or complaints beyond the spine, such as gastrointestinal or cardiopulmonary discomfort. A thoracic disc herniation can be included in the differential diagnosis of patients with negative gastrointestinal, genitourinary, and cardiopulmonary system basic studies.[18]
 |
 |
| Central Canal Stenosis | Lateral Recess Stenosis |
Stenosis
The term stenosis means narrowing of an opening. This can be at the foramen where the nerve runs through or spinal stenosis, which is narrowing of the spinal canal, resulting in symptoms and signs caused by compression of the vascular and nervous structures. Disc bulging, protrusion, and herniation combined with degenerative bone growth called osteophytes and changes of the facet joints can cause a narrowing of the spinal canal. Central spinal stenosis is found in almost a third of the population.
Symptoms of central spinal stenosis may be related to blood arterial flow, venous congestion, and increased pressure; the nerve roots can be irritated by local inflammation; or direct compression in the central canal that contains the spinal cord. Spinal stenosis is a disorder related to many factors, and symptoms can vary with or without pain in the buttocks or legs when walking, which disappears with sitting or bending forward and this is called neurogenic claudication.
Stenosis with claudication leads to a forward bent walking position and foot pressure measurements indicates risk of falls forward and to the symptomatic side in the elderly.[19] Central spinal stenosis resulting in radiculopathy is differentiated by pain on walking that is relieved by rest, the feeling that the legs are going to give away, a feeling of cold or numbness in the legs, a feeling that the legs are made of rubber and do not belong, and night pain that is relieved by walking. Radiologic evaluation often differentiates this from disc herniation.
Lateral recess stenosis with nerve irritation mostly presents without low back pain and rare muscle weakness. The pain may radiate into the ankle and occasionally into toes. Further, radiologic examination often differentiates it from a radiculopathy caused by disc herniation. In the illustration above, the lateral recess stenosis is caused by degenerative changes in the right facet joint, and these are often involved in a back pain condition called facet syndrome.
Multifidus Muscle Dysfunction

The lumbar multifidus muscles are on either side of the spine and play a significant role in lumbar spine function. Dysfunction of this muscle in back disc herniation has a negative affect on function and outcomes following lumbar disc surgery. The degree and presence of multifidus muscle dysfunction can aid in clinical reasoning for a rehabilitation regimen to restore the function of the lumbar spine.
The composition and structure of the muscle in patients with lumbar disc herniation and/or nerve root injury is noted to be a decrease in size and increase of the fat content. By using MRI images, fatty composition of the multifidus muscle at the same level and on the same side as herniation is found to be considerably higher than on the opposite side and has been shown to be a reliable reliable method of assessment
Both visual grading and quantitative measurement methods of the multifidus muscle demonstrated increased fat infiltration of the muscle on the same side as well as the the same level as the lumbar disc herniation. Additionally, fatty infiltration of the muscle was directly associated with both symptom duration and severity of nerve compression. Therefore, assessing fat infiltration is relevant and should be included in reprting.[20]
Fat infiltration of the multifidus with disc herniation indicates an inflammatory state of the muscle as well as the adipose tissue of the covering around the spinal cord.[21] The multifidus muscle has a significant role in spinal stability and is associated with fat infiltration and chronic back pain through loss of lumbar stabilization. A decrease in fat composition may show recovery and the rehabilitation strategies directed muscle activation and lumbar stabilization.[22]
Herniations at L3/4 and above are referred to as an upper lumbar disc herniation, which accounts for under 10% of lumbar disc herniations. There is a correlation between multifidus muscle degeneration and upper lumbar disc herniations. Lumbar muscle strengthening training may improve and prevent muscle loss atrophy and degeneration.[23]
Management Of Back Herniated Disc
Management of a painful disc, spinal stenosis, disc related pain, pain after surgery (post surgery syndrome) is mainly conservative care combining physiotherapy; traction, heat therapy, ice, back brace, electrical stimulation, exercise programs (back pain relief exercises, general back exercises), massage, safe manipulative therapy like Cox Technique, drugs for pain relief and inflammation are often employed. Injections may be recommended and surgery if these above conservative methods fail to provide relief for back pain or resolution.
 TENS Therapy
TENS Therapy Posture Braces
Posture Braces Ergonomic Aids
Ergonomic AidsSmoking And Disc Problems
Most specialists will indicate that nicotine from smoking decreases circulation in small blood vessels and this can have a negative effect on the disc. This makes sense because we know that smoking will decrease microcirculation, and some studies suggest a relationship between smoking and back pain. However, there is another reason that smoking may hurt the disc – coughing. Coughing can cause an increase in pressure on the disc. A cough can produce more pressure on the disc than lifting 25 pounds, therefore; having a smokers cough, a chronic condition from smoking, can actually damage the disc by trauma over a period of time. So, maybe it is a combination of coughing and decreased circulation.
In the study of vascular effects of drugs on molecular transport of disc and disc diffusion, researchers were surprised to find that nicotine actually had an effect of increasing blood vessels, however, it did not effect disc diffusion. So, it seems more likely that smoking damages the disc from coughing, rather than decreased circulation. Either way, it is probably a good idea to quit or at least cut down to protect the disc and help disc injuries heal.[24]
Serious Signs Associated With A Back Herniated Disc
The main concern is a cauda equina syndrome, which is a medical emergency requiring surgery. Though rare, cauda equina syndrome is a severe neurologic disorder that can lead to incontinence and even permanent paraplegia if left untreated. The individual nerve roots at the end of the spinal cord provide motor and sensory function to the legs and the bladder. The cauda equina (Latin for “horse’s tail”) refers to the sack of nerve roots with a common covering at the end of the spinal cord that is the continuation of these nerve roots in the low back region.
Cauda equina syndrome most commonly results from a massive disc herniation. Cauda equina syndrome has a range of symptoms, depending on the degree of compression and the nerve roots that are being compressed. Symptoms include severe low back pain, urinary or bowel incontinence, motor weakness or sensory loss in both legs, and saddle anesthesia (unable to feel anything in the body areas that would sit on a saddle). Symptoms may vary in intensity and come on immediately or evolve slowly over time. So, the warning signs include saddle anesthesia, recent onset of bladder dysfunction (such as urinary retention or incontinence), bowel incontinence and motor weakness in the lower extremity. Other conditions that may rarely lead to cauda equina syndrome include osteoporotic vertebral fractures and spinal stenosis.
Summary
A back herniated disc may range from an incidental finding on an MRI with no symptoms, an acute painful condition, to a chronic disabling problem, to a medical emergency. Most herniated discs do not require surgery and will resolve on their own or with conservative care measures. A herniated disc can be classic, with all the typical signs and findings or can be very elusive to diagnose from other conditions. Exciting new therapies like antibiotics, genetics and regenerative medicine associated with herniated discs may help lead the way for more effective therapies in the future.
Considering the importance of the deep lumbar muscles – multifidus, which are small muscles in layers that act to maintain segmental stability, maintain lumbar physiological curve, control facet joint movement, and adjust distribution of vertebral loads and pressures. Decline in function and fat infiltration places one at risk for problems. Here are some exercises to help in prevention and rehabilitation phase of recovery.
There is an association between major depression disorder and chronic lower back pain from disc herniation of the lumbar spine. It is associated with higher disability rates, socioeconomic disadvantage, and greater utilization of health care resources. Early detection and combined treatment of depressive symptoms is recommended.[25]
References:
1. J Spinal Cord Med. 2022 Mar;45(2):305-310
2. Int J Clin Exp Med. 2015 Feb 15;8(2):1634-44
3. Zhonghua Yi Xue Za Zhi. 2014 Jul 1;94(25)
4. Spine J. 2015 Nov 1;15(11):2360-8
5. Ann Rehabil Med. 2012 Feb;36(1):47-54
6. Eur Spine J. 2006 May;15(5):583-7
7. Spine J. 2020 Jul;20(7):1025-1034
8. J Orthop Res. 2021 Dec;39(12):2703-2710
9. Spine (Phila Pa 1976). 2013 Aug 1;38(17):1491-500
10. Global Spine J. 2015 Feb 25;5(5):360–365
11. Spine J. 2023 Sep;23(9):1375-1388.
12. J Pain Res. 2021 Jul 9:14:2095-2109
13. Asian Spine J. 2022 Apr;16(2):212-220
14. Clin Anat. 2022 Mar;35(2):204-210
15. Oncotarget. 2017 Jun 27;8(36):60558-60567
16. PLoS One. 2016 Nov 7;11(11):e0166031
17. Int J Rheumatol. 2020 Aug 29:2020:2919625
18. Case Rep Orthop. 2013:2013:621476.
19. Biomed Res Int. 2020 Jul 1:2020:5043583
20. J Int Med Res. 2019 Aug;47(8):3590-3600
21. Eur Spine J. 2021 Apr;30(4):837-845
22. Spine (Phila Pa 1976). 2021 Jan 15;46(2):129-130
23. BMC Musculoskelet Disord. 2021 Jan 19;22(1):92
24. J Orthop Res. 2014 Dec;32(12):1694-700
25. Int J Psychiatry Med. 2022 Mar;57(2):165-177