Schmorl’s nodes are a disc herniation into a spinal bone named after a pathologist late 1920’s
Where most disc herniations are associated with typical bulges, protrusions and extrusions that can place pressure on nerves resulting in back pain and sciatica, this type of herniation goes through the endplate covering the disc and directly into the bone.
A Schmorl’s node is typically found in the thoracic or lumbar spine (mid or lower back) and is most often not a major finding, as they are fairly common. However, after many years, we are still trying to learn the significance of these nodes. They are usually noted as a long-term finding without any symptoms and are found in about 30% of the population.
The location of upper lumbar prevalence may be explained by the endplates being stronger as you go down or caudal in the spine, thus the upper lumbar and lower thoracic spine may be more vulnerable to insults of the weaker endplates by Schmorl’s nodes. Regarding vertebral morphology or structure; there are also indications that the taller the spinal bone, the less strength it has to resist vertical forces, similar to wider discs being less resistant to torsional or rotational forces.
How Do You Get Schmorl’s Nodes?
Most can form after a heavy loading incident or trauma which forces the nucleus part of the disc through the endplate instead of the outer part of the disc. The outer part of the disc is normally more resistant to sudden forces than the endplate, especially in young individuals. Gymnasts show a high level of Schmorl’s nodes; think of a landing off the balance beam or a hard landing from a high ski jump, or taking a hard fall on your buttocks.
The location of most nodes indicate axial loading (vertical forces) are a major cause. When there is an injury that affects the spine in these up and down directions, nodes can occur. They will sometimes show edema (swelling) or a light area around the node. The edema may resolve in as little as 6 months, or may persist for some years. In some cases they are factors which can make the endplate and/or bone weaker and less resistant to structural failure, like bone diseases, degeneration, tumors or disc infection.
Not just a fracture to the endplate, but even a single impact injury without any structural damage can initiate degeneration of the disc through induced inflammation and abnormal energy metabolism of the disc cells.[1]
Are Schmorl’s Nodes Painful?
Not all Schmorl’s nodes are painful. However, endplates are meant to be intact in order to maintain the structural integrity of the disc and bone. Just like the outer part of the disc, structural failure can result in the inner part of the disc pushing into or through the outer part, known commonly as a disc herniation. Not all disc herniations are painful. They may not place any pressure on a nerve or on other sensitive structures, but damage is done to one degree or another.
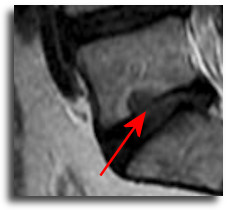
In a Schmorl’s node or intradiscal herniation, as the endplate cracks, some of the inner disc nucleus material goes through into the bone, like walking on a frozen pond and having your heel crack through the ice and the water seeping out. Typically the white area around the node is inflammation and this usually indicates a recent node from a trauma or injury. So, that is often painful. The pain is usually felt deep in the back and does not radiate into the legs like a typical disc herniation. It can be painful for a few years, then eventually calm down.
This is a reasonable, general line of thinking, however, some research indicates these to be a bit more consequential.
Painful Nodes
There are studies which indicate that Schmorl’s nodes that produce symptoms can be very painful, with high pain levels reported by patients as well as significant effects on quality of life.
Damage to the endplate can result in a loss of pressure to the inner part of the disc and placing more stress on the outer part, therefore, damage to the endplate can cause a series of mechanical and biochemical events that lead to degeneration and chronic back pain.
A node that has been chronic for some time, but no swelling noted, and then converts to swelling or modic changes around the node, along with typical herniation of the disc at that level, is highly suspicious of disc infection. A pathway for bacteria to enter the disc is associated with herniations that pull off a piece of the endplate. With a Schmorl’s node, there is already a pathway from the disc, through the endplate and into the bone. Any subsequent herniation, from either injury or age related degeneration may provide a direct connection, leaving the disc vulnerable to a rapidly progressing, pathological and deforming type of degeneration from low grade bacterial infection.
Even without infection, the inner part of the disc, when in contact with the blood supply of the inside of the bone can cause a significant immune response resulting in high levels of swelling, pain producing chemicals called cytokines, and high levels of pain which can follow a pattern of inflammation related pain of worse in the morning, better at noon, getting bad again in the afternoon, and worse at night. Morning stiffness is associated with lower back disc degeneration.[2]
If a node is not painful, it can produce symptoms if the nucleus keeps herniating more into the bone marrow. Once there is contact of the nucleus with the blood, an inflammatory immune reaction can result in pain and further structural damage to the bone itself as well as the disc.
 Traction & Inversion
Traction & Inversion Supports & Cushions
Supports & Cushions Belts & Corsets
Belts & CorsetsWhich Nodes Are Painful?
Because of the nature of the cervical spine with smaller bones and more mobility, of 582 subjects undergoing MRI for pathological signs of degeneration, only Schmorl’s nodes were consistently associated with neck pain[3]
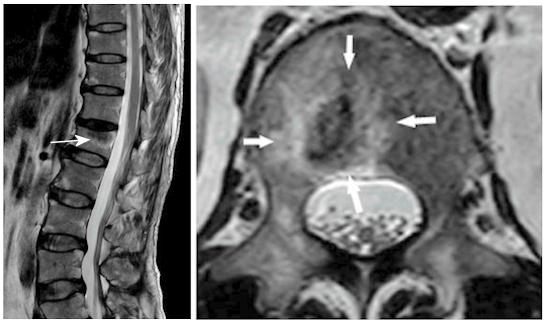
 There seems to be a pattern indicating a certain subgroup of nodes that cause back pain. These are ones that are only visible on MRI and follow the pattern of Type 1 Modic Disease in the bone around the node, indicating an active pathological process. Similar to modic type 1 changes, these indicate swelling and inflammation in the bone marrow. When this is seen, there is a high probability that the Schmorl’s node itself is a cause of pain. This may not be the main cause; often these are found with disc herniations or disc degeneration that can cause radiating pain as well as modic changes in the bone at other locations than the node. However, an active node would be a cause of pain as well.
There seems to be a pattern indicating a certain subgroup of nodes that cause back pain. These are ones that are only visible on MRI and follow the pattern of Type 1 Modic Disease in the bone around the node, indicating an active pathological process. Similar to modic type 1 changes, these indicate swelling and inflammation in the bone marrow. When this is seen, there is a high probability that the Schmorl’s node itself is a cause of pain. This may not be the main cause; often these are found with disc herniations or disc degeneration that can cause radiating pain as well as modic changes in the bone at other locations than the node. However, an active node would be a cause of pain as well.
Possible Consequences Of Active Nodes
When doing follow-up imaging studies, most nodes are stable. However, there is literature that indicates in about a year and a half, about 26% will increase in size and about 13% will show modic type 1 changes surrounding the node. It is also indicated that these active nodes may increase the risk of vertebral fractures by about 10%. Like modic changes, the invasion into the bone marrow produces microfractures as the bone surrounding the marrow becomes destroyed. Microfractures can produce a deep, sharp pain and can increase the swelling and inflammation.
Association With & Disc Degeneration
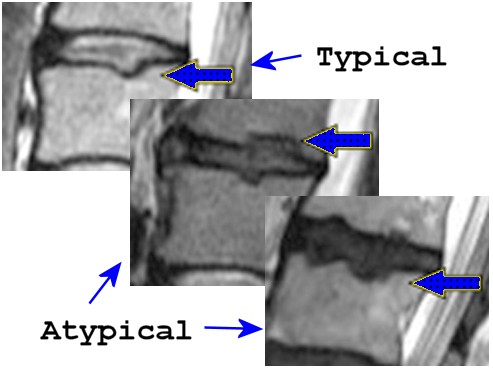
There is an association between lumbar spine Nodes and Disc Degeneration outlined in a large scale population based study using MRI. The authors found there are typical and atypical nodes with distinct characteristics. The atypical nodes appear either rectangular or irregular in shape, while typical are round. They found typical nodes were associated with 2 to 4 times the risk in severity of disc degeneration, while the atypical nodes were associated with a 5 to 13 times more severe degeneration. The study indicated atypical rectangular and irregular nodes were relatively uncommon, 6% and 4% respectively. They classified 4 different shapes: indented, round, sharp, irregular, and rectangular.[4]
There is a strong association between Schmorl’s nodes and degenerative spinal stenosis of the lumbar spine. This is a common problem seen in the older population and is the most frequent reason for spinal surgery in persons over 60 years old. The prevalence of lumbar spinal stenosis is about 47% in adults that have symptoms of numbness and pain being referred into the lower extremities.
 Massage Tools
Massage Tools Relief Supplements
Relief Supplements Topical Relievers
Topical RelieversIt appears that higher levels of spinal loading; higher BMI (e.g., weight gain during pregnancy), lifting heavy objects, and repeated bending and/or twisting movements can lead to disc endplate failure. This leads to disc herniation as seen with these nodes, buckling of ligaments that can protrude into the spinal canal as seen with loss of disc height, osteophytes or outgrowths of the spinal bone and joints, instability, and eventually lead to symptomatic degenerative stenosis.
The authors recommend health care professionals be aware of the connection between these nodes and stenosis. They recommend lumbar stabilization exercises may be useful in preventing or delaying stenosis as a consequence of Schmorl’s nodes.[5]
Nodes are associated with lower disc height, degenerative spinal stenosis, osteophytes, vacuum phenomenon (radiographic description of gas in the vertebral body), smoking and higher bone height.[6] Intradiscal vacuum phenomenon is closely associated with severe disc degeneration, Modic changes, and subchondral sclerosis (hardening and thickening of the bone beneath cartilage in a joint). This severely decreases the ability of bone to absorb stress as well as protect the disc leading to increased inflammation, altered disc nutrition, and enhanced disc degeneration. This possibly indicates long term effects of nodes.[7]
Schmorl’s nodes pathologies are underestimated in the cause of low back pain. Intervertebral disc degeneration at upper lumbar levels and end-plate disease at lower lumbar level in patients with low back pain are often seen. Higher degeneration and node scores are significantly associated with Modic changes at L4-L5 disc level. Nodes at L1-L2 or L2-L3 levels have approximately 7 times the increased risk of severe degeneration at the corresponding levels. The most significant factor associated with presence of nodes is the body weight of the patients and intensity of low back pain is associated with severe degeneration at the L5-S1 level.[8]
Treatment For Schmorl’s Nodes
Lumbar Spinal Decompression Devices
An acute node that is symptomatic can be treated similar to compression vertebral fractures. Initial conservative measures often consist of pain and/or anti-inflammatory medications, bed rest and external lumbar and/or thoraco-lumbar bracing. Heat and ice can be used accordingly and after the initial inflammation has subsided, some find spinal traction devices beneficial.
Chiropractic adjustments (I particularly like Cox Technique for this) and strengthening of supporting muscles may provide solutions. However, if these conservative treatments fail, nerve blocks and percutaneous vertebroplasty or kyphoplasty can be considered for relief prior to fusion surgery.
 New Mattresses
New Mattresses Heat Therapy
Heat Therapy Cold Therapy
Cold TherapyAgain, most of these are not pain producing nodes and are noticed upon examination of back pain from another cause. However, a small percentage of patients will have back pain that is not responding to typical therapies and have an MRI indicating a large node surrounded by bone swelling. In these cases, treatment is warranted. Indications are that vertebroplasty may be effective, especially when found with osteoporosis. Studies in using this cement type injection have reported about 80% success in these active schmorl’s nodes.
Percutaneous Vertebroplasty, often used to treat painful compression fractures, is a safe and effective procedure for Schmorl’s nodes that are symptomatic. It can be used for those who have not responded to conservative therapies or nerve/disc blocks. It is a procedure done under local anesthesia, where a type of cement is injected into the bone.[9]
Since Percutaneous Vertebroplasty (PVP) is a minimally invasive procedure, it may well be indicated before considering spinal fusion. Some surgeons may prefer Percutaneous Kyphoplasty (PKP), a slightly more involved procedure, where an inflatable balloon first creates a cavity in attempts for better cement delivery control and integration. Indications are the mechanisms for pain relief are about equal.
Nodes that are symptomatic can have pain similar to an acute compression fracture. MRI is indicated when CT and x-rays are unremarkable. MRI can show inflammation around painful nodes. Significant improvements are found for PKP, stabilizing vertebral integrity and maintaining functional improvements at 5 year follow up. PKP is concluded too be both safe and effective in those not responding to conservative therapy.[10]
Guided percutaneous vertebroplasty (PVP) can be used in the management of painful nodes. The cement is deposited in a cupule-like shape in fron and back of the node. There was 100% technical success, the average time for the procedure was 15 minutes, average amount of cement injected was 2.8ml, with significant pain decrease at 1 year follow up.[11]
While some may respond to conservative therapies like analgesics, bed rest, and external bracing, while waiting it out for a period of time to see if there is spontaneous healing, some may not obtain pain relief, therefore; surgical options (removal of the node with segmental fusion or less invasive procedures like vertebroplasty and nerve blockage), should be considered reasonable options.
Painful nodes can also be successfully treated with nerve/disc block under discography. This is an outpatient procedure where the nerves around the disc are heated by radiofrequency electrical current through a needle. This destroys the painful nerves. In a study, 89.2 percent noted improvement in their lower back pain.[12]
Active nodes in association with degeneration and instability may benefit from fusion surgery. Often discography is done to confirm pain at the level in question prior to any fusion. Good success rates have been noted regarding pain relief and increased functional ability with those who have active nodes with back pain not responsive to conservative treatment methods and who have a positive response to discography.
Discography is often used to determine the disc responsible for pain, but notes that the injection expands the disc space inducing endplate motion, and the entire functional spinal unit. Therefore, contribution from the associated facet joint and myo-tendinous insertions should also be considered.[13]
 TENS Therapy
TENS Therapy Posture Braces
Posture Braces Ergonomic Aids
Ergonomic AidsActive nodes have also responded to medications such as infliximab to reduce painful chemicals like TNF-α associated with marrow swelling. This medication is often used in rheumatoid arthritis. A case study found Infliximab infusions may be effective in treating chronic back pain with nodes. The authors recommended further studies based on their results. There are side effects that should be noted.[14] Anyone who is familiar with my articles on Modic changes should begin to notice a familiarity here.
Based on the similarity of active Schmorl’s nodes and modic changes, when found in association with typical disc herniation and additional signs of modic changes, antibiotics following the same protocol for modic changes may be a reasonable approach. Although studies are lacking, there is too much in common to dismiss this type of therapy in select patients.
A case report indicates a young patient that had nodes in the lumbar spine with signal changes in the vertebral endplate asociated with Modic I changes. The patient was successfully treated with antibiotics, rest and a back brace. The authors noted that two-directional Schmorl’s nodes (affecting both the upper and lower endplates of the same disc) may be infectious in nature.[15]
Summary
Schmorl’s nodes are most commonly found incidentally when investigating back pain, sciatica or some other cause and are not seen by many as related to pain, however, there is evidence supporting the damaging effects of active and/or large nodes regarding inflammation in the bone. In some of these cases, significant levels of chronic pain not responding to traditional therapy, progressive structural failure of the disc and bone, along with possible pathological fractures may result.
References:
1 Spine (Phila Pa 1976) 2022 Mar 1;47(5):E203-E213
2. Osteoarthritis and Cartilage Open 2024 Oct 18;6(4):100535
3. Fukushima Journal of Medical Science 2021 Dec 21;67(3):107-118
4 Osteoarthritis and Cartilage 2016 Oct;24(10):1753-1760
5. BMC Musculoskeletal Disorders 2017 Apr 20;18(1):164
6. BioMed Research International 2018 Nov 7;2018:1574020
7 Current Medical Research and Opinion 2022 Feb;38(2):255-263
8. Journal of Clinical Neuroscience 2022 Jun:100:66-74
9. Pain Physician 2017 Feb;20(2):69-76.
10. Medical Science Monitor 2017 Jun 13:23:2879-2889
11. Neuroradiology 2019 Apr;61(4):405-410
12 European Spine Journal 2018 Jan;27(1):13-18
13. Pain Med 2021 Aug 6;22(8):1735-1742
14. Rheumatology (Oxford) 2005 Dec;44(12):1588-90
15. Spine Surgery and Related Research 2018 Oct 19;3(2):193-195