
Are Modic Changes A Specific Disease Entity?
We have gone into details regarding antibiotics for back pain & how to determine if you may suffer from Modic changes, as well as frequently asked questions regarding the use of antibiotics for Modic changes type I. Let’s look at some of the evidence indicating Modic changes as a specific disease, rather than a normal finding of the degenerative spinal process.
A 2001 issue of The Radiology Journal noted that both moderate as well as severe type I and II endplate changes produced pain with disc injection discography 100% of the time.
A 2001 study in the journal Skeletal Radiology found an association between Modic changes and golf related low back pain, noting intradiscal steroid injections provided relief. Interesting study, however, only 4 patients were included.
In the 2006 European Spine Journal, the authors did a study on Modic changes and noted that the results indicate that Modic changes with disc degeneration is “an entity on its own”, and that it is different from disc degeneration without Modic changes. The authors further suggest that individuals with low back pain and Modic changes might deserve having a specific back pain diagnosis.
In a 2006 study in the German Journal RoFo, the authors noted that Modic changes in the endplate above the involved disc, especially those that are located in the center of the endplate, can indicate herniations that keep recurring and a sign of poor response to pain therapy.
Another 2006 edition of Rofo noted that Modic changes, especially those in the upper (superior) endplate of a herniated disc predicts a poor outcome to epidural injections. Epidural injections are often recommended for degenerative conditions associated with herniations, however, when Modic changes are involved, this may not be a wise approach. Injections in the disc (intradiscal injections) have been shown to provide better relief when Modic changes are present. Since Modic changes are a dynamic disease, showing changes from one type to another, intradiscal injections are not curative, but may provide temporary relief.
In the journal Spine, a 2007 study indicated Modic changes in the lower back, specifically at L5-S1 and Modic type I are significantly associated with low back pain & symptoms like sciatica, when compared to other locations in the lumbar spine as well as other types.
A 2007 study in the journal of Arthritis & Rheumatism found that high serum High-Sensitivity C-reactive protein (hsCRP) was able to differentiate Modic 1 changes from Modic 0 and 2; averaging 4.64 mg/liter for type I, compared to 1.33 mg/liter for Modic 0 and 1.75 mg/liter for Modic II.
A 2007 European Spine Journal study found that Modic 1 changes showed a tendancy to increase in frequency, are more associated with pain than Modic type II, and are strongly related to disc herniations in a 14 month follow up study. Therefore, those with lumbar disc herniation is a risk factor for developing painful Modic 1 changes during the following year.
A May, 2008 issue of the American Journal Of Radiology indicates Type I Modic changes are most likely inflammation and appear “strongly associated with active low back symptoms and segmental instability”.
The journal of Med Hypotheses in 2008 notes Dr. Albert and colleagues propose two pathogenic mechanisms for Modic changes: Mechanical Modic changes: The consequences of disc degeneration increase sheer forces on the endplates, resulting in microfractures and inflammation or leakage of toxic nuclear material through the microfractures. Infectious: Annular tear and subsequent herniation resulting in nuclear neovascularization, through which anaerobic bacteria find a pathway into the similarly anaerobic disc, thus producing a low virulent infection surrounded by resultant edema and inflammation.
The authors note that painful subchondral marrow signals are seen with spinal infections, osteoarthritis, as well as autoimmune diseases like spondyloarthritis and ankylosing spondylitis. Vertebral Modic changes are seen in relation to spondylodiscitis, fractures, severe degenerative changes, chymopapin injection, herniation and acute Schmorl’s nodes. Proposed methods of treatment for Modic changes would be related to the underlying cause, like specific rehabilitation programs, rest, surgery or antibiotics.
 A 2009 edition of the journal Radiology studied almost 2,500 discs, indicating that Modic type I changes are highly predictive of a pain generator. The term “highly predictive” is one that is not used lightly and must be supported by the evidence. This indicates that Modic type I changes are very likely to be the cause of pain.
A 2009 edition of the journal Radiology studied almost 2,500 discs, indicating that Modic type I changes are highly predictive of a pain generator. The term “highly predictive” is one that is not used lightly and must be supported by the evidence. This indicates that Modic type I changes are very likely to be the cause of pain.
The 2010 issue of the European Spine Journal studied what factors predicted the development of new Modic changes and determined the factors were related to the dynamics and status of the disc rather than the result of lifestyle factors like physical loading, smoking or gender.
A 2010 European Spine Journal studied pyogenic spondylitis in Modic 1 patients that had no signs of infection for 2 years. They considered the relationship between the two entities. They did frequent follow up studies including imaging and blood profiles indicating no abnormal blood profiles. It should be noted they performed C-reactive protein and not High-sensitivity C-reactive protein. Nonetheless, they noted in the 71 patients with Modic type I changes and without other signs of infection, pyogenic spondylitis was confirmed in 3 patients (4.2%). Noteworthy was 2 of the 3 had diabetes. The authors state this indicates it is important to consider pyogenic spondylitis prior to Modic 1 treatment.
In the May 2011 issue of Medical Hypotheses, the authors propose Modic 1 changes to result from an autoimmune reaction of the nucleus pulposus that has breached the endplate due to disruption from chronic and repeated shear forces. The subsequent outer annulus breach and production of inflammatory cytokines from the vertebral body in contact with the nucleus pulposus represents an autoimmune response resulting in bone marrow vascularization and edema, characteristic of Modic 1. They further postulate that clinical methods may used to circumvent this pain pathway.
A 2012 study in BioMed Central Medicine Journal found that exercise, a primary recommended therapy for back pain according to most standards, was not effective for those suffering from Modic changes.
A 1 year follow up study in the 2012 edition of the European Spine Journal noted that their study indicated Modic 1 changes may indicate a deforming and fast progressing pathological form of disc degeneration, comparing this to more normal age related and genetically determined degeneration. They noted different features of Modic changes compared to typical degeneration as deformation of the endplate, decreasing disc height and increased disc signal on MRI
A 2012 issue of the Global Spine Journal indicated that individuals with Type I Modic changes had a poor response to lumbar discectomy than those with Type II 1 year following discectomy, with higher rates of disability.
A 2012 edition of the European Spine Journal indicated, in a 14 month study, that Modic type I changes during the initial diagnosis was associated with poor treat outcomes and persisting low back pain at 14 months follow up, regardless of change in size of the type I lesions.
Does size matter? In a 2012 study in the journal Spine it was noted that size of Modic 1 lesions do not correlate with clinical symptoms. The main distinguishing feature for Modic lesions is the type, noting that when Modic 1 changes to a mixed M1/M2, clinical symptoms improve.
A study in a 2012 Annals of Physical and Rehabilitation Medicine noted better acute response to intradiscal injection for disabling chronic low back pain Modic type I over Modic II. The effects did not last greater than 6 months. The authors indicated side effects from cortivazol and triamcinolone corticosteroid intradiscal injections reported as disc destruction after puncture and disc calcification, a very painful condition. The authors used acetate of methylprednisolone or prednisolone, indicating no reported side effects for intradiscal injection of these or corticosteroids.
The authors indicate, “In contrast to other degenerative modifications of the spine, Modic type I changes are closely associated with chronic low back pain as suggested by observational studies”. They further note, “Taken together, our results and those of others strongly support the concept of a specific syndrome associated with Modic type I changes seen on MRI: worsening symptoms during chronic low back pain, inflammatory clinical and biological profile, and acute short-term response in pain level with intradiscal corticosteroid injection.” Part of their inflammatory profile refers to the 2007 study regarding serum elevated high-sensitivity C-reactive protein levels.
A 2013 study in the European Spine Journal indicated Modic 1 changes are responsive to a 100 day course of antibiotics for individuals suffering from chronic back pain. This is the study that so many have questioned and complained about. Despite calls from the authors to perform additional studies regarding antibiotics for Modic 1 changes, controversy remains and, to my knowledge, no additional studies have been undertaken to disprove the remarkable results. The only further evidence is through individuals in Europe that have undergone the therapy. These anecdotal reports confirm the results of the study as many individuals are reporting relief from chronic pain due to these specific Modic changes, resulting from the course of antibiotic treatment. These reports indicate that, while not everyone is a candidate for antibiotic treatment due to lack of Modic Type I changes, or have adverse effects/allergies to the Bioclavid/Amoxicillin Clavulanate; and not everyone who qualifies will respond due to strictly structural Modic 1 changes, response is generally very good in practice. Dr. Albert has made a significant contribution to the treatment of chronic back pain and disability.
A 2013 study in the European Spine Journal noted Modic type I changes related to a herniated disc may be due to inflammation surrounding an infected disc, finding Modic changes associated with discs that are infected with bacteria, as compared with those discs that are not infected.
The 2013 issue of Biomed Research International performed a study where they removed material from disc herniations. Their in-depth study was concluded by noting, “… the role of P. acnes in lumbar disc herniation should not be readily dismissed”.
 In the 2013 publication in Advances In Orthopedics, 88 patients received posterior dynamic stabilization surgery for chronic disc degeneration with Modic types I and II. This was a successful procedure for both types. The authors of this study stated that Modic 1 changes are associated with painful disorders connected with instability and painful disorders connected with instability. Although both types responded well to the surgery, Modic I were more unstable than Modic II, although Modic II can be associated with radiculopathy.
In the 2013 publication in Advances In Orthopedics, 88 patients received posterior dynamic stabilization surgery for chronic disc degeneration with Modic types I and II. This was a successful procedure for both types. The authors of this study stated that Modic 1 changes are associated with painful disorders connected with instability and painful disorders connected with instability. Although both types responded well to the surgery, Modic I were more unstable than Modic II, although Modic II can be associated with radiculopathy.
A 2013 issue of the Global Spine Journal noted in one of the largest population based studies, the findings of the authors indicate that Modic changes are “clearly associated with disc pathology” (degeneration, bulges/extrusions) …”and endplate abnormalities” (Schmorl’s nodes).
A 2013 issue of the Journal Of The Korean Neurosurgical Society studied Modic changes in the thoracic spine, finding them differing than cervical and lumbar spine in type and frequency, but noticing a strong relationship between thoracic Modic changes and disc herniation.
It is known that P. acnes is a problem with shoulder joint infections and device implant failures post-surgery. In a 2013 article titled, “Propionibacterium acnes: an underestimated etiology in the pathogenesis of osteoarthritis?”, the authors hypothesize that cycles of relapse and remitting pain in osteoarthritis is possibly related to bacterial flare-ups in the affected joint.
In the European Spine Journal, 2014, a study indicated heredity as a factor in Modic changes, indicating the heredity factor was approximately 30%. This is not surprising, considering the heritability associated with degenerative disc disease. So, with a family history of back problems, it may be a good idea to pay extra attention to avoid problems associated with chronic back pain.
In the 2014 edition of the journal Spine, a study indicated that disc herniations that occur when Modic changes are present respond poorly to conservative treatments and are less likely to reduce in size without surgery, showing greater signs of endplate involvement.
A 2014 issue of Postgraduate Medical Journal indicates that there may be an infective component involved indicating this may indicate “novel potential treatments” for those suffering chronic back pain not responding to other therapies.
The 2014 paper in Skeletal Radiology studied patients with radiculopathy due to a herniated dic, with and without Modic changes, for a period of 1 year. The results indicated Modic 1 changes can prolong sensory pain recovery in subjects with disc herniation related lumbar radicular pain.
In a 2014 issue of the European Spine Journal, Dr. Adams and colleagues noted that a herniated disc can pull away some of the underlying bone, thereby opening a pathway between the disc and bone, which can lead to inflammation of Modic 1 changes in the endplate and infection by bacteria in the disc.
A 2014 issue of the Global Spine Journal indicates that endplates are especially vulnerable to damage, and can cause communication between inflammatory disc chemicals with bone marrow. Damage to the endplates can be areas of “reactive bone marrow lesions” including abnormal nerve growth that is pain sensitive. The authors indicate the role of this type of endplate damage in back pain is under-appreciated due to the lack of clarity when visualizing diagnostic imaging.
A 2014 study in the European Spine Journal noted the effects of Modic changes in the cervical spine, indicating Modic changes in the neck were found in association with degeneration and stenosis – narrowing of the spinal canal. They also found altered angular motion in segments with Modic changes indicating restricted motion in cervical spine segments afflicted with Modic changes, which is opposite the findings of instability or excessive motion in the lumbar spine.
In a 2014 study in Spine, the authors noted higher disc degeneration and Modic changes with irregular endplates compared to concave or flat shaped endplates. They indicated Modic changes exhibited less angular motion with increased translational motion, relating pathological motion of the spine in relation to endplate shape and remodeling via kinetic MRI study of 2100 lumbar motion segments.
In the 2014 issue of the Spine Journal, the authors followed back pain patients over 1 year who were on sick leave for back pain and compared MRI findings, noting the only MRI finding associated with failure to improve symptoms and return to work were those with Modic 1 changes.
A case study presented in the 2014 journal of Skeletal Radiology, where the authors used intradiscal injections (inside the disc, not epidural) to treat a patient with Modic type I changes indicated total relief after 2 injections in the disc. Six months later, an MRI showed that the Modic type I had changed to Modic type II. A year after the first injections, the patient again experienced back pain and MRI revealed Modic type I changes that were worse than the first scan. (Not sure if it was an increase in grading and/or frequency, term used was “stronger”). Two more injections in the disc were administered which again relieved the pain. Six months later, MRI indicated changes back to Modic type II. The authors indicate Modic type I changes to be reversible local inflammation. This provides some evidence that intradiscal injections are preferred to epidural injections when Modic changes are involved, and that these injections are not curative, but do show positive results.
In the 2014 European Journal of Radiology, a scientific study was published indicating 346 individuals with symptoms directly related to lumbar disc herniation were significantly less likely to respond to imaging guided lumbar nerve root blocks if they had Modic changes.
In 2014, The European Spine Journal published a study where patients with disabling Modic changes undergoing surgery had biopsies to investigate the microscopic bone structure and formation associated with the different types of Modic changes. They found significant differences between the types. They provided microscopic evidence of type I with high bone resorption, reduced in type II and more stable in type III. They indicated “…Modic types represent different stages of the same pathological process linked to the adjacent disc.”
This is in basic agreement with biopsies done by Dr. Modic and colleagues, where type I were considered fibrovascular tissue, like fluid from a boil, indicating very active degeneration. Type II being a more stable, but chronic process with fatty replacement in the marrow, and type III being the most stable form with scar tissue or thickening.
A 2014 study in the Chinese Medical Journal noted that lumbar disc herniation with Modic changes and mainly back pain responded better to discectomy and fusion, rather than discectomy alone. This provided further evidence of the unstable nature of Modic endplate changes in that patients presenting with these changes respond more favorably to stabilizing fusion after discectomy as opposed to disc herniations without associated Modic changes.
In the 2014 issue of Trials, a prospective study involving pamidronate, a class of drugs called bisphosphonate, for Modic 1 changes is proposed for undergoing a trial. The authors note Modic 1 changes as “erosive degenerative disc disease”, with back pain relating an inflammatory pattern of pain, similar to diseases known as spondyloarthropathies like rheumatoid arthritis, ankylosing spondylitis and pain producing bone diseases like vertebral fractures and fibrous dysplasia, Paget’s disease. They are proposing a clinical trial of intravenous pamidronate. While this may be effective for some, this is serious medication with serious side effects. This is similar to a previous study using zoledronic acid, another biophosponate, where 95% of those taking experienced side effects. Improvement was noted, however, there was a small number of participants with Modic changes. Curiously, a history of studies involving Modic changes was outlined, however, no mention of Dr. Albert’s work with antibiotics was noted in this proposed trial of therapy for Modic changes.
The results of the study were published in a 2014 BMC Musculoskelet Disorders, where it was indicated that treatment reduced the intensity of low back pain short term as well a reduction of NSAID use over a one year period. Side effects prominent were fever, flu like symptoms and joint pain.
 In studying Modic changes, sometimes we will need to move beyond terminology. We know that Modic changes are diagnosed according to type. This is important in doing research and finding specific therapeutic measures, in consideration of the differences among types of changes on a subjective and objective basis. Understanding that diagnosing type depends on the MRI machine used. Low field MRI units are better at determining which type of Modic change exists. Some MRI machines will not show Modic changes. With the advent of high field units, classification of type becomes obscure and is generally noted as “endplate signal changes” or “reactive endplate changes”. While this does not allow typing and is insufficient for determining specific parameters relating to diagnosis and treatment of a particular type, it is sufficient to document the existence of Modic changes.
In studying Modic changes, sometimes we will need to move beyond terminology. We know that Modic changes are diagnosed according to type. This is important in doing research and finding specific therapeutic measures, in consideration of the differences among types of changes on a subjective and objective basis. Understanding that diagnosing type depends on the MRI machine used. Low field MRI units are better at determining which type of Modic change exists. Some MRI machines will not show Modic changes. With the advent of high field units, classification of type becomes obscure and is generally noted as “endplate signal changes” or “reactive endplate changes”. While this does not allow typing and is insufficient for determining specific parameters relating to diagnosis and treatment of a particular type, it is sufficient to document the existence of Modic changes.
A 2014 study in the Korean Journal of Spine indicated surgical fusion rates for those with Modic endplate degeneration changes were significantly lower than those without endplate degeneration. Regardless of Modic type, fusion was about 50%, however, without Modic changes, fusion rate was about 90%. Adding Alendronate (Fosamax), a bisphosphonate used in treating osteoporosis and indicated to possibly retard degeneration, had no effect on outcomes. Therefore, Modic changes suppress the fusion process for those undergoing Single Level Posterior Lumbar Spinal Interbody Fusion (PLIF).
Nonetheless, we are continuing to find evidence that Modic changes are a specific type of spinal disease regarding back pain. In the 2014 issue of the Spine Journal, it was clearly indicated that disc degeneration by itself is not associated with back pain relating to MRI findings, however, when combined with “endplate signal changes”, they are “highly associated with low back pain”.
An article published in the 2014 issue of PLoS One, they compared Modic changes in the lower back and neck of over 3,000 patients. They noted that the occurrence of Modic changes is “significantly higher” in those with neck and back pain. The authors defined Modic changes as “degenerative changes of the vertebral endplate”, and that they are related to minor endplate trauma due to repeated loading, or repeated injury to the disc. They also noted the inflammatory nature of Type I indicating “vascularized bone marrow and/or edema” (actually, neovascularization more accurately describes the infiltration of the marrow with blood vessels and unmyelinated or hypersensitive nerve fibers), type I “fatty change or necrosis of the endplate (this would be fatty degeneration of the bone marrow and cell death of the endplate), and Type III “endplate sclerosis” (scar tissue).
The authors additionally state, “Furthermore, clinical evidence suggests that Modic changes are often observed in people with neck pain” and indicate endplates are the “weak link” in the spine, which are subject to irreversible injury from repetitive or excessive loading. The endplates assist with vital nutrient transport to the disc and damage can result in loss of this nutrition and resulting accelerated degeneration. Since the neck is biomechanically subject to less loading than the lower back, Modic changes are more frequently seen in the lumbar spine than the cervical spine, however; both are directly related to spinal pain in their respective spinal locations.
A 2014 issue of the European Spine Journal indicated a study where 21 discs were surgically removed from patients suffering low back pain or sciatica as a main symptom. Almost half of the discs contained cartilage that showed signs of being pulled off from the endplate during herniation. The authors indicate that disc herniations frequently contain cartilage peeled from the endplate. These cartilage pieces are not readily absorbed and can increase the risk of long term sciatica. Furthermore, it was stated that this loss of cartilage from the endplate creates a pathway in the cartilage for inflammation and disc infection.
A 2014 European Spine Journal article studied the charachteristics of Modic 1 pain in 120 patients. The authors noted the presence of at least one of the three inflammatory pain patterns can be used as a screening tool to detect Modic 1 changes; 1) maximal pain on morning, 2) waking at night because of pain, 3) morning stiffness for longer than 60 minutes. This is also a characteristic seen with ankylosing spondylitis.
The authors also noted back pain with lumbar extension was associated with Modic 1, and the side of pain was associated with the side of the lesion found on MRI. They also indicated sedentary work was a protective factor, however, lowering loading and daily rest does not appear to be an effective strategy. They noted better results with oral steroids than NSAID’s.
A 2014 study in the American Journal of Neuroradiology used diffusion-weighted MRI (DW-MRI) to differentiate infectious from degenerative Modic changes type I. They found that a visible “claw sign” indicated degenerative changes, while the absence of this claw sign “…strongly suggests diskitis/osteomyelitis. The absence of the claw sign predicted osteomyelitis 100% of the time in 14 of 14 patients.
 I was very interested in this study titled, “Diffusion-weighted MRI “claw sign” improves differentiation of infectious from degenerative Modic type I signal changes of the spine”. Finally, a clear way to diagnose the difference. For a time, I recommended DW-MRI for Modic change diagnosis. All were showing claw signs? Perhaps since Modic changes represent a low-virulent infection, the distinction is not that simple. Well, I corresponded with one of the authors, Dr. Tanenbaum, to try to clarify this. He indicated, “…claw represents a border zone induration as a response to a slow degenerative process. Infection is presumed to advance more rapidly and thus not manifest the striking border zone changes. I would assume it applies to all infections but more experience is needed”.
I was very interested in this study titled, “Diffusion-weighted MRI “claw sign” improves differentiation of infectious from degenerative Modic type I signal changes of the spine”. Finally, a clear way to diagnose the difference. For a time, I recommended DW-MRI for Modic change diagnosis. All were showing claw signs? Perhaps since Modic changes represent a low-virulent infection, the distinction is not that simple. Well, I corresponded with one of the authors, Dr. Tanenbaum, to try to clarify this. He indicated, “…claw represents a border zone induration as a response to a slow degenerative process. Infection is presumed to advance more rapidly and thus not manifest the striking border zone changes. I would assume it applies to all infections but more experience is needed”.
On further questioning, he stated “My presumption is that type I changes are more indolent Than infection and thus create the claw”. Thus, a claw sign may still represent Modic 1 changes related to bacterial infection. However, this would differentiate symptomatic Modic 1 due to osteomyelitis from Modic 1 structural or bacterial related, an important finding related to emergency treatment and possible lives saved, considering some of the grave consequences of osteomyelitis. We do know from a previous 2010 study, that 4.2% of Modic 1 patients were diagnosed as having pyogenic spondylitis, even without signs of infection. Perhaps in those with diabetes, DW-MRI would be prudent.
A 2015 issue of the journal Spine studied the difference between high and low field MRI for degeneration in the lumbar spine. They used low field (0.25T) and high field (1.5T or 3.0T) MRI systems. They found that there was very good agreement between disc herniation, foraminal, central canal and lateral recess stenosis and nerve root compression. However, no mention of Modic changes was noted. The authors indicated the low field produced more artifacts from motion, presumably due to longer scanning time. We know 3.0T systems are not good for Modic changes, however, they could have included reactive endplate changes.
Thus, we will see more general descriptions of Modic changes as high frequency units are being promoted as better than low field. In my experience, high field units may show greater detail regarding disc herniations or extrusions, however, noting Modic or endplate changes without the ability to type these changes is a distinct disadvantage for those suffering particularly from Modic Type 1 changes; the most painful and inflammatory type. When Modic Type I changes are suspected via history, a low field MRI unit should be used in order to recommend treatment; antibiotics have only been proven to be effective for Modic Type I, and to document objective findings related to a patient’s complaints for medical and/or medico legal purposes.
If Modic 1 changes were found, would there be clinical reasoning for prescribing exercise, or would this be contraindicated? Are you doctors prescribing physical therapy paying attention? Are you P.T.’s paying attention? Or just getting paid? Would even a more generalized “reactive endplate changes” provide clear evidence for a pain generator and/or offer an explanation for chronicity other than central sensitization? Maybe if we use 3.0T units, Modic changes will just go away! The authors of the above study indicate high field is just as good as low field for “most” findings in degeneration; perhaps suggesting high field is better due to less motion artifacts, while ignoring what is probably the best finding in relation to chronic back pain from degeneration.
A 2015 study in Cell Biochemistry and Biophysics found patients with lumbar herniated discs that were treated conservatively for 6 months were less likely to have the disc heal when Modic changes of the endplates were present. This relationship was noted by the authors as “strong”. The authors further indicated those with Modic changes had significantly more cartilage in the herniated disc tissue along with less vascularization and macrophage levels, which helps explain delayed healing.
A review was published regarding back pain in relation to low grade bacterial infection in a 2015 BMC Medicine Journal . The authors reviewed the literature and determined there was a moderate level of evidence indicating back pain due to Modic 1 change with disc herniation and bacterial infection regarding causation as well as relationship.
The authors indicate a greater understanding regarding the evidence from the study by Dr. Albert is necessary to justify a change in practice. They further reiterate significant concerns regarding antibiotic resistance. They additionally call for more studies, something Dr. Albert has called for years previous in her original study. I think time and resources would have been better spent actually doing a study rather than a review of studies already done. There will always be suspicion of cross contamination. The issue of antibiotic resistance has been addressed regarding this self-limiting process again and again. Evidently, the need to unnecessarily alarm and revisit this issue will be a never ending process, regardless of the status of the evidence and the nature of this moderately evident disease process.
If they are not going to do studies, a theory should be posed as to the results of Dr. Albert’s study and a new mechanism proposed for the specific antibiotic (Augmentin/Bioclavid) producing such results in a specific population group. I guess we need absolute evidence to consider a change in thinking for a specific group of back pain sufferers. You would think they were talking about anyone with back pain. We know it is a group of patients with chronic back pain, a specific history, suggestive subjective findings, along with very specific objective findings. Perhaps if they are looking for a greater understanding of the evidence, they should have taken her certification course instead of looking at search strategies. It would seem the number of Modic Antibiotic Spinal Therapy (MAST) clinics, as well as their success in treating these patients have indicated the evidence is clear and practically justified.
The Royal Australasian College of Surgeons published a review in the 2015 ANZ Journal of Surgery. They reviewed current literature about the hypothesis on bacterial infection causing disabling lower back pain and radiculopathy. It is a very interesting article and well done, however, most of the article tries to relate consensus regarding cultures of bacteria, for which there are none. A nice review of the techniques and conflicting results, however, no conclusion can be drawn. They seem largely focused on herniated discs, while relegating Modic changes as a possible, unproven relation.
 They state, “Low-grade anaerobic bacterial infection of the intervertebral disc is a hypothesis that has challenged the status quo of the pathogenesis and treatment of lumbar disc herniation.” I do not know of anyone proposing antibiotics for disc herniations. The protocol used by Dr. Albert had strict criteria, including those with a specific subset of disc herniation related to a specific subset of Modic changes, related to specific clinical and history subjective/objective findings. Understandably, the authors state, “..antibiotic resistance is a major developing problem around the world and, if used inappropriately, the proposed 100-day course of oral amoxycillin/clavulanic acid has the potential to greatly influence this increasing level of resistance further.
They state, “Low-grade anaerobic bacterial infection of the intervertebral disc is a hypothesis that has challenged the status quo of the pathogenesis and treatment of lumbar disc herniation.” I do not know of anyone proposing antibiotics for disc herniations. The protocol used by Dr. Albert had strict criteria, including those with a specific subset of disc herniation related to a specific subset of Modic changes, related to specific clinical and history subjective/objective findings. Understandably, the authors state, “..antibiotic resistance is a major developing problem around the world and, if used inappropriately, the proposed 100-day course of oral amoxycillin/clavulanic acid has the potential to greatly influence this increasing level of resistance further.
Therefore, sufficiently accurate diagnostic tools would be needed to prevent patients complaining of back pain associated with lumbar disc herniation from unnecessarily protracted courses of antibiotics prior to considering surgery.” I would agree, should the assumption be treating everyone suffering disc herniations with antibiotics, however; revisiting this, for what is proposed as a very specific subset of chronic back pain patients with a self limiting disease is not contributing to anything, but needless alarm. Similarly, the pros and cons of current culture methods also is non-contributory. Obviously, new techniques need to be developed and we can argue about conflicting results till then.
They further state, “More specific predictive factors and factors that could be used at the time of diagnosis are needed before a protracted oral antibiotic regime could be considered for use beyond the research field.” Well, there are specific subjective and objective findings already being used successfully, beyond the research field, into direct clinical practice.
Additionally, they conclude, “Promising results in support of the disc infection hypothesis have been published, but it is obviously too early to drastically alter one’s practice.” I am not sure of who is demanding a drastic alteration in anyone’s practice. I do not think it is asking too much to consider a course of antibiotics should a patients history not contraindicate antibiotic use, and specifically indicate a correlative history, along with both subjective and objective findings typical of one suffering from chronic, disabling Modic 1 related back pain, with or without radiculopathy. I don’t think this self limiting disease poses a threat to a global antibiotic resistance disaster.
The authors conclude, “Although definitive evidence is lacking, the disc infection hypothesis has the potential to cause a paradigm shift in the approach to back pain caused by HNP [herniated nucleus pulposus] and as such should not be dismissed lightly.” I think they have done a brilliant review, however, their premise is misguided. It should not be dismissed lightly in consideration of Dr. Albert’s double blind study and the numerous and growing Modic Antibiotic Spinal Therapy Centers treating a very specific subset of disc herniation.
Motion characteristics of Modic changes in the lumbar spine were featured in a 2015 Journal of Neurosurgery Spine. The authors studied 450 patients with back symptoms focusing on the biomechanics of Modic changes as compared with other conditions using a special weight bearing kinematic MRI. They found a significant association between increased translational motion (instability), especially with type I, and a decrease in angular motion in accordance with increasing Modic changes. The authors indicated Modic changes, a disorder of the endplates, may significantly impact segmental spinal stability.
A 2015 study in the European Spine Journal found that osteoclast activators are elevated in discs with Modic changes. The study involved disc specimens from herniated disc tissue. The authors noted the relationship between the cytokine tnf-α and Modic changes. The authors indicated factors secreted by disc tissue stimulates osteoclasts, and this is involved in the process of Modic changes.
Osteoclasts break down bone, degrading bone matrix and dissolving mineral. Normally, there is a homeostasis between the activity of osteoclasts and osteoblasts, which build bone. An imbalance in this mechanism can result in conditions like osteoporosis. This is an interesting article that begs further study. Tnf-α can cause formation of osteoclasts. It is produced in reaction to toxins by pathogens or immunological substances and is related to rheumatoid arthritis, an inflammatory and destructive bone and cartilage disease. This could also relate to a problem with the bone marrow cells which inhibit osteoclast formation or tnf-α mediated destruction of osteoblasts and interference with their differentiation. So, we are looking further into Modic changes and the relationship between their known association with tnf-α, bone marrow changes and inflammation.
Of note, in a 2015 study in the German journal Zeitschrift für Orthopädie und Unfallchirurgie, the authors focused on adjuvant antibiotic therapy for spondylodiscitis cases treated surgically. The prominence of age distribution was significant for 60 to 80 year olds, 55% in the lumbar spine. 60% of the patients had not been diagnosed or received any treatment for 1 month. Almost 50% had coexistence of diabetes mellitus.
A 2015 study in Spine indicates that high levels of multifidus muscle fat infiltration was related to severity of back pain and disability, while high levels of fat infiltration of the erector spinae muscle was related to decreased disc height and Modic changes. This is an interesting finding and the authors postulate a possible cause or effect relationship in regards to structural features of disabling low back pain for future studies.

Fatty infiltration of paraspinal muscles is a known degenerative feature of spinal disorders. Previous studies have indicated this in osteoporosis, facet joint arthrosis and whiplash injuries with poor functional recovery. I have not seen a correlation between this and Modic changes previously. A causal relationship seems unlikely, however; it is reasonable to assume an effective relationship at this point, as well as an area of interest in the future, perhaps another factor related to MRI field sensitivity.
A 2015 study in the journal BMC Musculoskeletal Disorders followed low back symptoms and Modic changes over a 2 year period. The authors confirmed the nature of Modic 1 changes being positively associated with pain and disability, as well as decreasing pain and disability with change to Modic 2. The authors of the study found a significant association between Modic 1 changes and low back pain and disability. They conclude, “These results lend support to the hypothesis that LBP patients with M1 represent a specific subgroup of patients with LBP.”
A 2015 study in the journal Spine followed twins for 10 years and indicated that Modic changes are an independent risk factor for episodes of severe and disabling back pain. The authors call for additional studies to identify the histology of Modic changes.
A 2015 study in the American Journal of Roentgenology found that patients who underwent microdiscectomy for herniated disc with surgically confirmed endplate cartilage herniation were associated with Modic changes on MRI. Modic changes were located at mid endplate level and posterior corners. Other MRI findings associated with cartilaginous endplate disc herniation were posterior osteophytes, posterior marginal nodes, mid endplate irregularities and extruded material with a heterogeneous low signal intensity.
In 2015, a study in the journal European Radiology investigated long term improvement of pain reduction with indirect cervical nerve root blocks while comparing MRI findings at the location of steroid infiltration. Those with compression of the nerve root had good long term outcomes, while those with extrusions showed less improvement and were four times more likely to undergo surgery compared to those with protrusions. The authors further noted, “There are less improvement in patients with Modic type I changes”.
A 2015 review and meta-analysis in the journal Spine sought to determine a possible relation between low virulent disc infection and development of symptomatic disc degeneration. The authors did a comprehensive search using six electronic databases and concluded “…the possibility that disc infection may be linked with disc degeneration should not be ruled out”. They noted those with symptomatic disc degeneration were 6 times more likely to suffer from a disc infection, the major culprit being Propionibacterium acnes.
A 2015 study in the European Spine Journal found Indian Hedgehog (ihh) protein was positively correlated with severity of cartilage degeneration in both types 1 and 2 Modic changes. Indian Hedgehog signaling is related to tumorigenesis and arthritis; as serum levels have been found to respond to anti-tnf-α therapy in ankylosing spondylitis, affecting functional target genes in the Hedgehog expression pathway.
The authors indicate blocking the ihh pathway may be of therapeutic value in cartilage endplate degeneration; however, a safe delivery system targeting ihh signaling remains elusive. Fibrocartilage and enthesis (specialized tissue attaching tendon to bone) development are related to Hedgehog responsive cells and are modified by loading. SMO
A 2015 review in Annals of the Rheumatic Diseases suggests Modic 1 changes to be a particular “phenotype” or “biomarker” of non-specific chronic low back pain, and an anatomical lesion with specific biological, radiological and clinical features. The authors indicate an active discopathy with local inflammation related to predisposing genetic factors and biochemical or mechanical stress, as well as local infection. The authors indicate Modic 1 changes are of “high clinical relevance”.
A 2015 study in the journal Orthopedics followed over 1200 patients who had microendoscopic discectomy for disc herniation, over a period of 10 years. Significant risk factors for re-operation, in addition to the level of degeneration and degeneration next to the level of microdiscetomy, those with Modic type I were almost 15% more likely to require re-operation within the period observed than those without. For Modic type II, only about 4% difference was noted.
A 2015 study in The Spine Journal did a large study on Modic changes of the lumbar spine of over 1,500 individuals. The authors noted that Modic changes were associated with Schmorl’s nodes, disc degeneration and disc displacement at the level affected. Type 1 were less than half prevalent than type 2 and were more strongly associated with disc displacement and a large affected area. The authors concluded that Modic changes are “…significantly associated with disc pathology and endplate abnormalities”
A 2015 European Spine Journal study found that Modic 2 changes had a significant impact on axial pain symptom intensity at one year follow up for those undergoing single level anterior cervical discectomy with fusion surgery, and also negatively influenced adjacent segmental degeneration.
A 2015 study in the journal BMC Musculoskeletal Disorders used lumbar facet joint injections to see if Modic changes would effect outcomes of this therapeutic approach. Although the patients were not diagnosed as having facet joint pain nor pain from Modic changes, the authors noted approximately 40% of patients without Modic changes had clinically relevant improvement, whereas approximately 33% with Modic changes had improvement 1 month after injection. They noted a tendency for better outcomes in those without Modic changes for a non-specific diagnosed group of patients, using a technique usually reserved for specific diagnoses. Very curious study.
A 2015 paper in the journal European Cells & Materials studied the effects of inflammation on disc degeneration. The authors state, “In spite of the controversial nature, subclinical bacterial infection of endplate/vertebrae and/or discitis as a cause for disc degeneration and LBP warrants further consideration and careful investigation.”
The comprehensive article further indicates, “These clinical studies suggest that anti-cytokine therapies as well as, in a subset of patients, antibiotic regimens hold promise in treating low back and radicular pain.”
In consideration of some of the rapid deleterious effects produced by inflammatory chemicals like TNF-α, the authors stress, “In light of this evidence, the timing of targeted anti-inflammatory treatment modalities is likely to have a critical impact on overall efficacy and success of therapy.”
A 2015 study in the Spine Journal was one of the largest studies with MRI to assess Modic changes in the lumbar spine. The authors indicated Modic changes were associated the severity and presence of low back pain as well as disc degeneration. The authors concluded, “Our study further stresses the significance of MC (Modic changes) as important imaging phenotypes associated with LBP [low back pain].”
In yet another attack on MAST (Modic Antibiotic Spinal Therapy) is presented in a 2015 Discovery Medicine Review. While the authors indicate the growing interest in antibiotics for symptom producing disc degeneration, they indicate, “… the notion that subclinical anaerobic bacterial infection could play a role in symptomatic disc degeneration”. I think a review of the literature above by any reasonable scientist suggests more than a “notion”. Another attempt to massively expand what is a specific subset of back pain sufferers.
The authors indicate Dr. Albert’s study is “…is one of the most strikingly successful experimental treatments for LBP [low back pain] to date.” I agree, however, they proceed to indicate “shortcomimgs”, and “possible confounding effects of amoxicillin-clavulanate.” They indicate evidence of clavulanic acid’s anti-inflammatory effect in ulcerative colitis and it’s analgesic effects in mice undergoing morphine withdrawal. However, Dr. Albert chose this based on recommendations from well noted microbiologists as the antibiotic of choice with the least ant-inflammatory effect. Additionally, it does not explain the long term effects, many months and in cases years after the antibiotic has been stopped. Perhaps more information is forthcoming with a clinical trial on antibiotics & Modic changes using a single dose amoxicillin, without clavulanic acid.
Again, these authors revisit the “antibiotic resistance” controversy; something that has been addressed ad infinitum here and elsewhere, however, it must be the politically correct thing to say in order to maintain the controversy.
 Evidently, in their conclusion, the authors are concerned that antibiotics should not be the only focus of attention for inflammatory back pain conditions. Honestly! Who would have guessed there were other causes? Metabolic syndromes? Aberrant mechanical loading? I don’t mean to be facetious here, it is a very well written and informative article; the authors do a great job of indicating mechanisms of disc inflammation, along with a fantastic graphic on signaling pathways. I very much enjoyed reading it. However, it could have done without the obvious negative references to Dr. Albert’s work.
Evidently, in their conclusion, the authors are concerned that antibiotics should not be the only focus of attention for inflammatory back pain conditions. Honestly! Who would have guessed there were other causes? Metabolic syndromes? Aberrant mechanical loading? I don’t mean to be facetious here, it is a very well written and informative article; the authors do a great job of indicating mechanisms of disc inflammation, along with a fantastic graphic on signaling pathways. I very much enjoyed reading it. However, it could have done without the obvious negative references to Dr. Albert’s work.
A 2015 study in the European Spine Journal found that disc samples obtained from patients undergoing discectomy indicated that the bacteria P. acnes is found significantly more in herniated discs with annular tears than in those without annular tears. The authors indicate from control muscles samples that a true infection is far more likely than previously indicated contamination. This indicates that P. acnes (Propionibacterium acnes) can access the disc via tears in the annulus fibrosus.
A 2016 review in the European Spine Journal noted bone marrow lesions seen on MRI as Modic changes present a high specificity for low back pain of disc origin. The authors indicate that Modic types indicate stages of the same pathological process, characterized by inflammation, high bone turnover, and fibrosis. They indicate a disease model where predisposing factors are related to an autoimmune response to disc material or discitis.
Regarding treatment, the authors indicate no consensus and relate non-surgical options as antibiotics, intradiscal injections, bisphosphonates, and anti-TNF-α; antibody. The authors concluded, “Modic changes are likely to be more than just a coincidental imaging finding in LBP patients and rather represent an underlying pathology that should be a target for therapy.
In a 2016 International Orthopaedics review, the authors indicate Propionibacterium acnes to be an opportunistic pathogen causing infections, such as joint and bone infections, implant device infection, central nervous systems infection, synovitis, osteitis, hyperostosis, as well as acne, pustulosis and prostatitis. It is also strongly correlated with spondylodiscitis, pyogenic discitis and vertebral osteomyelitis.
“Specially, patients can attain significant relief of low back pain, amelioration of Modic changes and alleviation of sciatica after antibiotic therapy, indicating the role of P. acnes in these pathological changes.”
The authors noted possible routes for disc inoculation related to Modic changes: 1) Via the circulatory system when skin or mucosa is broken and neovascularization is found around a disc when the annulus fibrosus is breached. (2) Via the circulatory system where macrophages devour P. acnes, transport into intervertebral discs and release viable bacterium upon cell death. They indicate macrophages aggregate around the ruptured annulus after disc herniation where some may contain devoured bacteria.
The authors related candidates for antibiotic therapy should; (1) Have low back pain for greater than 6 months with failed exercise therapy; (2) more than 1 or 2 years with a herniated disc; (3) Modic type I changes at the level of the herniated disc. They further suggest rifampicin as an alternative or in combination with ß-lactam antibiotics, such as amoxicillin, due to its effectiveness against P. acnes and its capabilities for soft tissue and bone penetration.
A 2016 pilot study in Biomed Research International isolated P. acnes from a Modic 1 disc and inoculated discs of rabbits. The P. acnes group developed Modic 1 changes along with degeneration. They also inoculated S. aureus into the rabbit discs. Comparing the results, S aureus discs showed typical signs of a pyogenic infection, while the P. acnes displayed a latent low grade chronic inflammation. The authors postulated varying degrees of virulence with different species of P. acnes. The S. aureus rabbits displayed pyogenic discitis consistent with spinal infection where we commonly see fever, body weight loss, and abnormal ESR. S. aureus rabbits also displayed higher death rates.
The authors concluded that according to Koch’s Postulates, P. acnes was strongly correlated with Modic changes and disc degeneration. “In clinical practice, one should be more aware of the presence of P. acnes in patients with Modic changes and disc degeneration.”
A 2016 study in the Asian Spine Journal found a correlation between low levels of vitamin D and Modic changes in 316 patients with chronic low back pain. Deficiency of vitamin D is known to cause neuromusculoskeletal pain. Vitamin D is involved with decreasing inflammation by regulating cytokines. Joint pain and fatigue are associated with low vitamin D levels. It is essential for normal function of muscles, nerves and bone. Although the causal relationship is yet to be established, the authors state, “We feel that studies on symptomatic improvement of back pain and potential reversal of Modic changes upon treatment with vitamin D may be warranted.”
A 2016 study in the Journal of Manipulative and Physiological Therapeutics applied spinal manipulation to patients with disc herniations and Modic changes. The noted improvements in patients with Modic Type II was significantly better than those with Type I. The authors noted that Modic 1 patients were significantly less likely to indicate improvement at 1 year; attributed by the authors to being prone to “relapse”. Therefore, we continue to see evidence that symptoms of Modic 1 Changes are quite resistant to traditional therapies. There is no indication of follow up MRI at 1 year. It is also not clear if relapse indicates specific exacerbation of chronic disc herniation or a relapse in symptoms related to inflammatory fibrovascular tissue, which implies improvement within maximum benefit at some point.
A 2016 study in the Journal of Orthopaedic Research isolated P. acnes from a human disc with Modic 1 changes was injected into discs in rat tails. Within 14 days, fibrotic tisue was absorbed into the bone marrow, TNF-α was identified at the marrow/disc junction, and MRI revealed Modic 1 like changes in the bone marrow. The authors concluded that P. acnes proliferates within the disc and induces reactive degenerative marrow changes visible as Modic 1 changes.
A 2016 study in the journal Medicine related specific findings or imaging biomarkers in Modic changes to low back pain of a prolonged and severe nature as well as disability. The authors found type II to be more than twice as prevalent as type I. In general, Modic changes were found in those who were older, had more disc problems, and more disc degeneration than those without Modic changes.
Where the standard grading system is based on the depth of changes on MRI, this study found the length of visible changes were significant; with changes along 2/3 or greater of the length of the vertebral bone to be correlated to more prolonged severe lower back pain and disability. They found Modic 1 was more strongly associated with pain than type II, and a greater number or frequency of Modic changes found increased the above associations.
A 2016 study in European Spine Journal found at 1 year follow up that persisting Modic 1 changes with a decrease in disc height and an increase in endplate lesions are associated with persisting pain, disability, and may be signs of prolonged chronic low back pain with a deforming degenerative process. Therefore, the authors indicate this should be a factor leading to specific treatments and early intervention that can affect the process.
A 2016 study in the Spine Journal examined inflammatory chemicals called cytokines and Modic 2 changes. They found a significant increase in many of these cytokines associated with Modic 2. The authors stated “These results further strengthen the association between MCs [Modic changes] and low back pain”. It should be noted that Modic 1 changes are significantly more associated with inflammation than Modic 2.
A 2016 study in PLoS One evaluated discs using biofilms and found an 11% prevalence of abundant P. acnes in 290 patient discs undergoing surgery for herniations. The authors introduction noted Propionibacterium acnes to be a slow-growing, fastidious, gram positive, facultative anaerobic bacteria found in acne, device related and post-operative infections. P. acnes have additionally been withing in the gastrointestinal tract, oral cavity, genitourinary tract, external ear canal, conjunctiva of the eye, and may also play a role in conditions, like prostatitis, sarcoidosis, SAPHO (Synovitis, Acne, Pustulosis, Hyperostosis and Osteitis – an auto-inflammatory disease), and degenerative disc disease.
In their conclusion, the authors indicate “Because ‘finding abundant microorganism in organisms suffering from the disease’ is one of the most important of Koch’s postulates, in judging the relationship between a specific microbe and a specific disease, we believe that our findings support the theory that P. acnes is involved in the pathogenesis of at least a subset of patients with degenerative disc disease.”
A 2016 article in the journal Future Science OA follows the progression of Modic changes from an innocuous “normal finding” of degeneration, to documentation of an infectious pathway in disc disease. The literature is reviewed in a clear, concise manner, indicating an “…imperative to continue researching the utilization of antibiotic treatment for this condition”.
The authors elucidate the alternative to the mechanical/degenerative pathway. Bacteria of low virulence enter the disc after traumatic tears in the annulus or disc herniation. This process can tear fragments of the end plate which delays resorption of the herniation and causes neovascularization. Bacteria, most often different subtypes of P. acnes, are transported in the circulatory system from skin or nonskin origin that have the ability to colonize intradiscally. What follows is inflammation and rapid degeneration with end plate damage. Modic changes are seen on MRI and pain, often locally and 24/7, and disability result in many cases. The protocol of antibiotic therapy provides a 50% pain reduction in 50% of patients with Modic 1 changes following disc herniation.
A 2016 study in the journal Spine examined 169 discs harvested from 87 patients undergoing either cervical or lumbar spinal surgery. They found positive cultures in 45% of the discs using biofilms. By contrasting discs from controls versus those suffering dicogenic pain and disc herniation, there was a significant association of positive bacterial cultures with disc herniation. The authors of this study concluded “Endemic bacterial biofilms are significantly associated with IVH [cervical & lumbar intervertebral disc herniation] and discogenic pain.”
A 2017 study in BMC Musculoskelet Disorders compared Modic 1 changes with discs less tan and greater than 50% disc height. They found that those with less than 50% disc height tended to be young males at the L5/S1 level, while those with greater than 50% tended to be older females at the L4/L5 level, and associated with greater osteophyte formation. Th authors postulate whether this represents continuing stages of the same process or a specific phenotypic subsets of Modic 1.
An interesting quote from the background section of the article, “Modic 1 signal changes detected on magnetic resonance imaging (MRI) encompass clinical, radiological and biological features, which allows for defining a specific subgroup of patients with chronic low back pain (cLBP).”
A 2017 study in the European Spine Journal examined the relationship between bone marrow and disc in Modic changes. The authors note Modic changes are bone marrow lesions that can be a diagnostic indicator for discogenic low back pain. The authors found pro-osteoclastic changes in discs of Modic 2, an inflammatory dysmyelopoiesis (aberrant morphology that can result in poor blood cell production) with fibrogenic changes in the marrow of both types, and up-regulation of neurotrophic receptors in the bone marrow and discs of both types (I & II). This give insight into the cellular processes and pain generating factors in Modic changes.
In a 2017 Journal of Neurosurgical Science, the authors did a pilot study to see if Modic 2 changes are associated with low grade infections. They compared tissue cultures in patients having elective surgery for low back pain without Modic signs (23) to those with Modic 2 changes (16). Intra-operative culture examinations indicated positive results in 6 of 16 (37.5%) Whereas those without Modic 2 changes had positive cultures in 1 of 23 (4.3%). The study, although limited in scale, does support a hypothesis where some Modic 2 changes may be related to low virulent bacteria.
A 2017 study in the Hong Kong Medical Journal examined data from 126 patients who underwent discectomy for lumbar disc herniation. 101 initial and 25 re-operation for recurrance. The authors examined criteria for recurrent disc herniation at a single L4/5 level. They noted a review of literature indicated recurrance rates between 5 and 15%.
They noted body mass index, gender, age, smoking, diabetes mellitus, herniation type, preoperative radiological parameters Pfirrmann disc degeneration grade, disc height, Modic endplate changes, duration of symptoms and, surgical technique. Out of all factors considered, they found that greater endplate Modic changes, higher body mass index, and preoperative higher disc height are important factors in recurrent lumbar disc herniation.
In a 2017 study published in the American Volume of the Journal of Bone and Joint Surgery, the authors studied the effects of direct inoculation of P. acnes in the spine from a rabbit model. They injected bacteria versus sham injection of a saline solutions. Modic change developments were investigated with MRI before the operation, 2 weeks, 1, 2, 3, and 6 months after the operation.
Those receiving the P. acnes inoculation showed significantly increased signal intensities at 6 months. Positive cultures showed higher prevalence of Modic changes, significantly increased expressions for tumor necrosis factor-α, interleukin-1β, and interferon-γ following injection of P. acnes The authors concluded that low back pain and disc degeneration are associated with Modic changes and the study results indicate Modic changes can be associated with P. acnes.
The authors of a 2017 study in the journal Spine induced Modic changes by injecting Propionibacterium Acnes into rabbit discs. This appears to be an extension of the above study with the exclusion of one author and going an additional 3 months. MRI evaluations were done at intervals up to 9 months along with tissue studies.
At 4.5 months 11 of 20 discs were type I, at 9 months 9 of 20 discs were type II. T1 signals significantly decreased from 3 months, while T2 was significantly higher at from 3 to 4 months, then decreased dramatically at 6 to 9 months. Real time polymerase chain reaction indicated significant up-regulation of inflammatory cytokines in the endplates, while histological studies indicated abnormal endplates, disc degeneration, inflammation and micro CT confirmed bone resorption. The authors noted P. acnes is capable of surviving in the end plate and initiating inflammatory responses that present as type I and II Modic changes that are time dependent.
A 2017 study in World Neurosurgery found that percutaneous endoscopic lumbar annuloplasty and nucleoplasty provided favorable outcomes for patients who did not respond to conservative treatments for disc related low back pain. However, it was noted that Modic changes were significantly related to poor results.
A 2017 study in the journal BMC Musculoskelet Disorder found a single intravenous infusion consisting of 5mg of zoledronic acid, a bisphosphonate, promoted a trend towards conversion of type I to type II at one year as indicated on MRI. For the zoledronic acid treatment group, type I decreased by 11% with a slight decrease in symptoms, where the placebo group there was an increase in type I by 18% and an increase in symptoms. Bisphosphonates are more commonly used to treat high calcium levels in the blood seen with bone damage certain cancers, multiple myeloma, destructive arthritis, Paget’s disease and osteoporosis. They also reduce inflammation. Some common used brands are: Zometa & Reclast
A 2017 study in the Korean Journal of Spine found associations between Modic changes and degeneration of the cervical spine , predominantly type II at the C5/6 level. The authors noted those with Modic changes had a higher grade of disc herniation, increase loss of disc space and a greater loss of lordotic curvature. They also noted a significant greater likelihood of fusion surgery in those with Modic changes.
A 2017 study in the European Spine Journal attempted to scrutinize the relationship between Modic changes and cervical spine instability, as well as the relationship to the normal lordotic curve and range of motion. The authors discovered. The authors found out of 464 patients observed, 94 had Modic changes, the most common location was the C5-C6 vertebral segment. They found instability was significantly higher in the Modic changes group. They also noted less curvature and motion range. They indicated cervical instability, less range of motion and curvature were risk factors for Modic changes. Cervical instability may result from cervical spine Modic changes.
A 2017 study in the Journal of Pain Research noted axial neck pain is often reported by patients as pain, stiffness, or dullness. The authors indicate degenerative disc disease is a significant risk factor for axial neck pain. Discs, muscles, and facet joints may contribute to symptoms. Modic changes are frequently found in association with with axial neck pain. Cervical kyphosis, a reversal of the cervical spine affects spinal motion and may cause spinal cord compression. It is an important risk factor for advancing disc degeneration and patients with this condition are at risk to develop neck pain as well as neurologic deficits. The study found Modic changes are associated with axial neck pain in those patients with cervical kyphosis.
A 2017 study in the Journal Of Orthopaedic Science found a higher risk of of pyogenic discitis, mostly Staphylococcus infection, after surgical laminectomy of the lumbar spine in those with Modic type I. Infection was related to the level of Modic I changes. The authors recommend pyogenic discitis, in which the usual symptoms are not yet manifest, should be ruled out carefully in patients with Modic type I to prevent one of the most serious complications following spine surgery.
A 2017 study in the Asian Spine Journal found Modic changes in approximately 13% of the 809 patients population. The study identified genetic polymorphisms of MMP20 and VDR were significantly associated with Modic changes. The authors noted a previous study, where 831 twins indicated a 16-43% prevalence of heritability of Modic changes.
The authors indicated the cause of Modic changes is still not known, and describe mechanical, infective, and biochemical theories. 1) With disc herniation and neovascularization, anaerobic bacteria can infiltrate into the endplates causing inflammation and edema. 2) Increased levels of inflammatory mediators, such as proinflammatory cytokines and interleukins have been detected in endplates, indicating an inflammatory cause. 3) With disc degeneration, increased stress on endplates results in fissures and microfractures which could be a major cause.
A 2017 study in the European Spine Journal concluded the response of disc cells to the bacteria P. acnes is associated with the presence of Modic changes. The bone marrow cells displayed an inflammatory response to P. acnes metabolites and disc cytokines. The results indicated a low virulent P. acnes disc infection to be a possible exacerbating factor to Modic changes.
 Another 2017 study in the European Spine Journal found an association between latent Propionibacterium acnes infection and chronic inflammation in degenerated discs, primarily in the disc containing visible bacteria, manifesting in increased numbers of neutrophils and cytokines. There was more severe degeneration in discs with P. acnes postulated to be from and bacterial induced inflammation.
Another 2017 study in the European Spine Journal found an association between latent Propionibacterium acnes infection and chronic inflammation in degenerated discs, primarily in the disc containing visible bacteria, manifesting in increased numbers of neutrophils and cytokines. There was more severe degeneration in discs with P. acnes postulated to be from and bacterial induced inflammation.
A 2018 study in Emerging Microbes & Infections found that P. acnes induces intervertebral disc degeneration by promoting nucleus pulposus cell apoptosis, concomitant with severe intervertebral disc degeneration. P. acnes was found to activate autophagy, likely to play a role in apoptosis of nucleus pulposus cells. Their findings validated the involvement of P. acnes in the pathology of disc degeneration, providing evidence that P. acnes induced nucleus pulposus cell death is likely responsible for the pathology of degenerative disc disease.
A 2018 study in the European Spine Journal found that positively charged antibiotics penetrate the disc better than negatively charged ones for treatment of low virulence disc infections. The authors (15 of them!) found clindamycin penetrated the disc better than cefazolin.
These authors note that P. Acnes found in disc specimens “exacerbate the pathology of degenerative disc disease”. They further state, “This hypothesis, therefore, raises the exciting possibility that antibiotics could play an important role in treating this debilitating condition.”
Let me get this straight, they are “excited” that antibiotics may treat disc disease? Where have they been? We know that the annulus of the disc is neutral and the nucleus is negatively charged. P. Acnes is negatively charged. We know that other factors like pH can effect charge. Amoxicillin is positively charged and has been specifically used in studies regarding this “debilitating condition”.
In fact, as early as a 1994 study in the journal Spine, it was concluded, “Our data suggest that penetration and distribution of antibiotics into avascular intervertebral disc is significantly influenced by the charge of antibiotics.”
There was also a nice 2016 study in the Journal of Biomechanics, “Kinetics of charged antibiotic penetration into human intervertebral discs: A numerical study.” The authors indicate, “Our results showed that the electrical charge had great effects on kinetics of an antibiotic penetration into the IVD; with higher concentrations and uptakes for positively charged antibiotics than those for negatively charged ones.”
So, the 15 authors of the 2018 study above conclude, “Positively charged antibiotics appear more appropriate for future studies investigating potential options for the treatment of low-virulence disc infections.” In case you were wondering why it takes so long to make progress.
A 2018 study in the journal Scientific Reports found a strong association between Modic change and vertebral endplate defects in the general population. After examining over 8,000 endplates from 831 twin volunteers. The authors indicate supporting evidence for endplate defects as an initiating factor in Modic changes and disc degeneration.
The evidence supports the hypothesis, however; we know that endplates are stronger as you move caudally down the spine. So, endplates at L1-2 are weaker than at L4/5. We know that Schmorl’s nodes, most prevalent in the upper lumbar region, do not necessarily lead to Modic changes in the vertebrae; sometimes around the node itself. We also know that the wider the disc, the weaker resistance to torsional forces. Therefore, Modic changes, being more prevalent in the lower lumbar region, may perhaps be better hypothesized as being initiated from the disc itself; tears and/or herniations.
A 2018 study in the journal World Neurosurgery found that “Severe disc degeneration in the lumbar spine is closely associated with Modic changes, and fatty infiltration in the multifidus and erector spinae muscles.”
A 2018 study in the Journal of Pain Research found that neck pain symptoms were more likely to be found after disc surgery and fusion in those diagnosed with Modic changes. This along with segmental kyphosis or loss of the normal relationship between the spinal segments are considered risk factors for ongoing axial pain after surgery.
A 2018 study in PLoS One indicates the possibility that P. acnes activates pain receptors by secreting toxic proteins called hemolysins which target and disrupt nerve cell membranes. The authors indicate postulate this may be involved on some level in symptoms and also the pathological process of chronic low back pain associated with P. acnes disc infections.
A 2018 study in The Spine Journal suggests that Modic type 1 changes result from an autoimmune response in combination with other inflammatory factors. The authors indicate that the autoimmune response is due to contact between the nucleus pulposus cells of the disc with bone marrow cells.
They indicate this process cannot trigger Modic changes without additional inflammatory stimulus and requires end plate defects that permit contact between the cells in addition to an adjacent inflammatory Modic changed disc, which amplifies the immune response.
A 2018 study in the American Journal of Neuroradiology found an association between Propionibacterium acnes in the discs of the cervical spine and Modic type I changes.
A 2018 study in the European Spine Journal suggests the lumbar Modic changes come first, then the P. acnes causes problems due to it’s metabolites inflammatory response to disc and bone marrow cells. This indicates that the infection exacerbates an existing Modic changed disc.
A 2018 study in BMC Musculoskeletal Disorders validated the presence and association of low-virulence anaerobic bacteria, mainly P. acnes in discs associated with Modic changes. The authors concluded, “Therefore, low-virulence anaerobic bacteria may play a crucial role in the pathophysiology of MCs and lumbar disc herniation.”
A 2018 study in the Journal of Spine Surgery confirms DWMRI can differentiate between type I changes due to degeneration (claw sign) and type I changes due to infection (no claw sign). No excuse for future studies to not use DWMRI in patient selection and evaluation. Failure to do so will result in questionable findings and a failure to differentiate between infectious or non-infectious cause. Obviously, there is no reason to use antibiotics for strictly mechanical causes.
A 2018 study in the Journal of Orthopaedic Surgery and Research found asymmetrical Modic changes in the cervical spine were most common at the C5/6 level and associated with poor response to conservative treatment. They were also associated with disc herniation and neurological symptoms. Surgical outcomes were satisfactory.
A 2019 study in World Neurosurgery found by MRI evaluation that only the extent of Modic I changes were associated with pain severity and significantly associated with disability, whereas findings such as disc height, number of Schmorl’s nodes, Pfirrmann graded disc degeneration, and cross sectional area of lumbar muscles were not.
A 2019 study in the Journal of Orthopaedic Science evaluated cervical spine Modic changes over a 20 year period. Type II was the most common, followed by Type I, then Type III. The most affected segment was C5/6 and was associated with disc protrusion and neck pain.
There was an association with disc degeneration and neck pain, however, the authors found no correlation with arm pain or numbness, shoulder stiffness, age, BMI or smoking.
This is all fascinating information and great studies. However, where are the practical implications for symptoms, diagnosis and treatment? Do we just continue researching the biochemistry? From what I see; we have antibiotic therapy documented through Dr. Albert’s work – I see nothing to refute her work or results since her double blind study, and I do not see further clinical trials and studies published by other authors using this method, which is very curious at least. With the advent of DWMRI differentiation regarding infection vs mechanical, patient selection can be significantly improved.
We have biologicals (certolizumab, etanercept, adalimumab, infliximab…) which have some positive documented therapeutic evidence. Certainly, there are more risky side effects associated with these drugs, however, it is either an alternative or first choice depending on patient factors. And we have surgery, which indicates the alleviation by removing the problem and/or fixating instability.
There is another option, do nothing! Just wait, eventually it will change to a more stable and sclerotic type III. Forget about the costs to society in terms of human suffering and lost productivity.
A 2019 study in the Journal of Medical Genetics identified a genetic correlation with Modic changes in an intron of the PTPRD gene that may act via the development of cartilage or nervous system. The authors indicated Modic change as a distinct phenotype of disc degeneration presenting as a pathological marrow signal change on MRI. They noted a strong association with back pain with a heritability of about 30%.
A 2019 study in the European Spine Journal used weight bearing MRI to indicate the areas of Modic I change increased with standing compared to lying down face up, and that this change significantly correlated with increased pain in the standing position.
There was moderate correlation between lower disc height and increased area of change, and very low correlation between increased area of change and the grade level of disc degeneration.
There has been a recent trend to eliminate Modic Antibiotic Spinal Therapy in the literature and I address the latest 2 studies in a separate article. This article outlines the scare tactics being used along with updates in techniques and directions for the future. I will continue to post non-biased literature here.
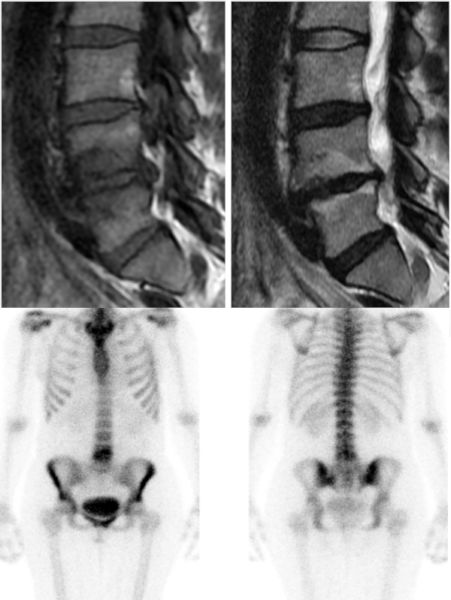 A 2019 study in the Asian Spine Journal the prevalence of paraspinal muscle fatty degeneration directly correlates with the presence of Modic type I and mixed I/II change in patients with low back pain. The association also included a decreased cross sectional area of the muscles.
A 2019 study in the Asian Spine Journal the prevalence of paraspinal muscle fatty degeneration directly correlates with the presence of Modic type I and mixed I/II change in patients with low back pain. The association also included a decreased cross sectional area of the muscles.
This confirms previous studies indicating fatty degeneration of the paraspinal muscles in association with Modic changes.
Paravertebral muscles have a very important role in lumbar spine stability The grading system used was: grade 0, normal; grade I, minimal focal or linear fat deposition; grade II, up to 25%; grade III, 25%-50%; and grade IV, more than 50%.
Another 2019 study in the Asian Spine Journal studies the effects of common degenerative findings and back pain. Change in the shape and intensity of nucleus pulposus, decreased disc height, disc herniation, vertebral endplate changes, presence of osteophyte, and posterior high intensity zones are degenerative changes often found in imaging studies. In the study, most findings were weakly associated with pain. However, “Modic type 1 change, disc extrusion, and disc sequestration were associated with LBP [low back pain] in most subjects.”
Interestingly, the study includes Modic I in the category with the most extreme forms of disc herniations regarding pain.
A 2019 study in Pain Physician used percutaneous endoscopic lumbar discectomy with a transforaminal approach (TF-PELD) to treat lumbar disc herniations. This is a minimally invasive technique that seeks to preserves the stabilizing elements of the spine and minimize the manipulation of surrounding tissue, reduce postoperative pain, and decrease complications. The authors noted postoperative back pain and functional status trended toward deterioration with in patients with Modic type I signals.
A 2019 study in Biomed Research International examined risk factors for early recurrence after lumbar discectomy. There were many factors analyzed in the study to arrive at a scoring system. Among the factors, Modic changes were studied. They found that Type I was 25%, type II was 14.3%, type III was 33%, with no Modic change at 8.27%.
Type I and III were significant predictive factors and among the highest percentages of risk factors analyzed. Type III was highest as the disease progresses to a state where the most damage is seen regarding trabecular bone fractures, thus indicating the importance of addressing early Modic changes to minimize damage as well as risk factors for possible future procedures like discectomy.
A 2019 Review in the European Spine Journal indicates lack of reporting guidelines hinders interpretation and comparison of findings for Modic changes. The authors conclude, “Thus, it is critical to adopt imaging and reporting standards that codify acceptable methodological criteria.” This is a call to action and I agree with the authors that it is “critical” at this point to have “…reporting that will allow for better integration of research into this LBP phenotype.”
A 2019 study in the Journal of Orthopaedic Translatation harvested endplates from patients undergoing surgery for spine fractures or fusions and found Lubricin is present in lumbar endplates where it may have an anti-inflammatory function. The authors noted P. acnes infection inhibits lubricin in cartilage endplate cells which may facilitate the progression of Modic Changes and endplate degeneration.
A 2020 study published in Cureus compared low back pain patients who has at least two magnetic resonance studies between 2013 and 2016. The first study MC [Modic changes] were in 283 out of 774 vertebrae (37%), where the second follow-up, MC was observed in 343 of 774 (43%) vertebrae [actually 44%]. New MCs were observed in 59 vertebrae [8%]. The authors noted 2 patients showed complete resolution of MC in the second study [0.26%].
The authors concluded, “In our retrospective case-control study, we have found that MCs can transform into different types or disappear completely over time. [They did not mention – or increase in number (8%) compared to ‘disappear’ (0.26%)] A significant positive correlation was found between the presence of MC type 1 changes in the visual analog scale(VAS).” [A well established fact as is transformation of type]. Normally, I would not post this, but it shows we need better work than this study.
A 2020 study in European Journal of Radiology Open found that bone scintigraphy (scan) showed significant increased uptake for type I (93%) and type I mixed changes (64%) compared to other and their mixed types (5%). It is visible as a hot spot with increased tracer uptake related to bone blood flow, especially to osteoblast activity, so it shows physiological activity of an osseous lesion.
A 2020 study in Neurospine examined the effects of Modic changes of the cervical spine on outcomes of anterior cervical discectomy and fusion surgery (ACDF). The most common type was II, located at C5/6 level, generally older patients, required bigger fusions, and had longer duration of symptoms before surgery. The authors concluded, “While MC may not affect specific outcomes following ACDF, they may indicate a more debilitating preoperative state for patients.” They also noted changes at C7/T1 level did display greater disability levels following surgery.
A 2020 study in the European Spine Journalfound Modic I disability grade of low/moderate in 22% of patients and high in 88%. The authors concluded that, “The discs with Modic I MRI signal could represent potential targets for medical treatments, whereas Modic II seems to be a more likely point of no return in a degenerative process. Note: The study included 20 patients.
A 2020 article in Medical Hypotheses considered hyperbaric oxygen treatment (HBOT) as a complementary Treatment for Modic changes. The authors indicated, “As an adjuvant treatment administered in combination with systemic antibiotics, HBOT could increase the sensitivity of Propionibacterium acnes to antimicrobial drugs under hyperoxic conditions, resulting in faster MC resolution. Overall, the faster infection resolution, diminished bacterial load, and anti-inflammatory effects due to reduced cytokine expression and levels of infectious by-products could lead to faster pain resolution following HBOT, and a significant improvement of quality of life in these patients.”
A 2020 study in the journal Spine found any Modic change and type I were associated with prolonged disabling low back pain. Additionally, changes covering the whole anterior and posterior direction or the whole endplate, as well as the height, were significantly associated with prolonged disabling low back pain. The authors concluded, “Our study showed a significant and independent association between MC [Modic changes] and clinically relevant LBP [low back pain].
A 2020 study in Journal of Orthopaedic Surgery and Research found recurrent lumbar disc herniation (rLDH) occurs frequently after percutaneous endoscopic lumbar discectomy (PELD) when Modic changes (MCs) are present. The authors concluded, “If we choose PELD for patients with MCs, we need to inform these patients that they have a higher incidence risk of rLDH, especially for old patients. They also found if cartilage is present in the herniated disc component, these patients should also be informed of a higher risk of recurrent disc herniation, possibly requiring a second operation.
A 2020 study in the International Journal of Molecular Sciences Indicates vertebral endplate bone marrow lesions/Modic Changes on MRI are associated with chronic low back pain and may be underdiagnosed due to guidelines against routine spinal MRI in primary care. They found serum biomarkers related to type III and type IV collagen, molecules in bone marrow fibrosis, were associated the presence of Modic changes. They concluded, “Bone marrow fibrosis may be an important pathophysiological process in MC that should be targeted in larger biomarker and treatment studies.”

A 2020 study in the European Spine Journal indicates preoperative Modic changes and severity of endplate damage are independent risk factors for developing postoperative surgical site infection. The authors concluded, “MC could be foci of chronic subclinical infection and not mere markers of degeneration, as initially described.”
A 2020 study in the International Journal of Spine Surgery used 16s DNA sequencing in patients with chronic low backache and Modic changes (MC) finding 13.5% had elevated leucocytosis, 28.6% with raised erythrocyte sedimentation rate, 72.7% showed high quantitative C-reactive protein, and 90% of the disc samples showed presence of bacteria in PCR study.
The authors targeted the conserved gene of the bacteria (ie, 16s ribosomal DNA) and used a universal eubacteria nested-amplification protocol that may detect picograms of bacterial DNA. They concluded, “MC may have an infective etiology.”
A 2021 study in BMC Musculoskeletal Disorders found patients undergoing surgery for thoracic myelopathy due to ossification of the ligamentum flavum had poorer outcomes with concurrent lumbar stenosis and thoracic Modic changes.
A 2021 study in the European Spine Journal indicated, “Lumbar Modic change (MC) can serve as a diagnostic marker as well as an independent source of chronic low back pain (CLBP)”. They assessed blood serum biomarker profiles and found that IL-1sRII and HGF (hepatocyte growth factor) were elevated among MC patients with CLBP, regardless of MC type or size, compared with asymptomatic controls.
A 2021 study in the Global Spine Journal concluded, “Preoperative Modic changes in lumbar disc herniation is associated with less favorable back pain, functional scores and patient satisfaction in patients undergoing microdiscectomy.”
A 2021 study in the International Journal of Molecular Sciences indicates, C. acnes can stimulate the expression of a host of inflammatory molecules previously associated with pathological changes in disc tissue, including neo-innervation. “While still controversial, the role of C. acnes in DDD remains biologically credible, and its ability to cause disease likely reflects a combination of factors, particularly individualised response to infection.”
A 2021 study in World Neurosurgery evaluated 527 patients. Severe disc degeneration was detected with Modic changes through the whole end plates at L4-L5 (90%) and L5-S1 (88%) levels. The L5-S1 level had significantly lower lumbar lordosis. In the conclusion the authors state, “Severe IVDD was significantly more common in patients with Modic changes through the whole end-plate and in those with Modic type I changes.”
 A 2021 review in Clinical Spine Surgery notes type 1 Modic changes have been strongly associated with inflammation and severe LBP with etiologic theories like autoimmunity, mechanics, infection, and genetic factors.
A 2021 review in Clinical Spine Surgery notes type 1 Modic changes have been strongly associated with inflammation and severe LBP with etiologic theories like autoimmunity, mechanics, infection, and genetic factors.
The authors conclude, “With the aging nature of the population, MC has emerged as an extremely prevalent issue. Research into the pathogenesis of MC is important for planning preventative and therapeutic strategies. Such strategies may include rehabilitation, surgical fixation, stabilization, steroid or cement injection, or antibiotics. Improved diagnostic methods in clinical practice are thus critical to properly identify patients suffering from MC, plan early intervention, and hasten return to functioning.”
A 2021 review in The Spine Journal concluded, “In patients for whom other therapies have failed, and who might otherwise progress to disc replacement or fusion surgery, antibiotic therapy may be an attractive option.”
A 2021 Review in Future Sci OA indicates, “Newer and more advanced technologies clearly point to an ongoing low-grade infection. We have reviewed all of the clinical trials published in the recent past and conclude that there is compelling evidence for the effect of long-term oral antibiotic treatment for this patient group.”
The authors indicate that new compelling microbiological studies of the past 5 years, along with enhanced imaging technologies, have caused a better understanding of definitively demonstrated infectious pathway. The patient groups is chronic back pain, failure of conservative treatments and Modic changes type 1 on their MRI.
A 2021 study in The Spine Journal noted Patients with modic changes form a distinct clinical subset with reports of higher intensity of pain, poor clinical and surgical outcomes and higher incidence of recurrence, and an independent risk factor for increased post-operative surgical site infection. They found modic changes are associated with activation of intense inflammatory and host defense response pathways from proteomic analysis.
A 2021 study in BMC Neurolology indicates Modic changes seem to indicate a chronic irritating inflammation response and strongly indicates that refinement of our current treatment approach is needed and that radiculopathy patients should be further sub characterized based on their inflammation status.
A 2021 study in the European Spine Journal found Modic changes significantly influences disc inflammation and influences a pathological inflammatory state. It altered protein expressions resulting in a down-regulation of pathways involved in detoxification of reactive oxygen species, complement system and immune system. Results were verified by Immunohistochemistry with CD68 cell counts.
A 2021 study in Pain & Therapy concluded “Type I/II Modic changes in the lumbar region are significantly associated with LBP”. This was a large population-based study of 952 participants (second Wakayama Spine Study) and most noted for pain at L2/3 and L4/5 levels.
A 2021 review in Insights into Imaging is a radiologists perspective on spinal disorders mimicking infection. The authors indicate that degenerative spinal disorders in the inflammatory stage (Modic 1) can mimic infection particularly because of overlapping clinical presentation (acute spinal pain and inflammatory laboratory findings). They note vertebral endplate changes are related to inflammation mediated active disc degeneration, however, increased vascularity seen in Modic 1 predisposes to “non-specific, low-grade bacterial infections.”
This leads to indicating that Modic I changes are a risk factor for a non-specific (specified in the literature) bacterial infection. This leads to the question, how does an infection “mimic” and infection? And poses the question, which comes first, the chicken or the egg? It is important to distinguish between a potentially life threatening infection and a low grade infection. The authors discuss distinguishing features and the contribution of advanced techniques, like DWI and dual-energy CT(DECT).
A 2021 study in the European Spine Journal found an association between preoperative Modic changes and total endplate damage score greater than 6 to be associated with postoperative surgical site infection. The authors state, “MC could be foci of chronic subclinical infection and not mere markers of degeneration, as initially described.”
A 2021 review in the European Spine Journal noted evidence for infection in intervertebral disc degeneration and Modic change. The authors concluded, “Evidence to date implicates C. acnes identified through culture, microscopy and sequencing, with some suggestion of diverse bacterial colonisation in the disc.”
A 2022 study in Scientific Reports notes Modic I has an immunological component, involving autoimmunity or low-grade bacterial infections in the intervertebral disc, triggering a detrimental cascade of inflammation in the vertebrae. They indicated systemic gene expression suggest that immunological processes, particularly interferon signaling, are important players in the underlying pathobiology of these patients.
A 2022 review in Clinical Spine Surgery indicates Modic change (MC) has a strong association to low back pain. The authors concluded, “Research into the pathogenesis of MC is important for planning preventative and therapeutic strategies. Such strategies may include rehabilitation, surgical fixation, stabilization, steroid or cement injection, or antibiotics. Improved diagnostic methods in clinical practice are thus critical to properly identify patients suffering from MC, plan early intervention, and hasten return to functioning.”
A 2022 study in The Spine Journal found facet joint injections were significantly less effective when Modic 1 active endplate changes were found. Clinically meanigful back pain reduction was reached significantly more often in the absence of active endplate changes (73%) compared with patients with active endplate changes (35%).
A 2022 study in PLoS One indicates C. acnes is widespread in herniated disc tissues and different types of C. acnes could induce different Modic changes by increasing matrix metalloproteinase expression.
 A 2022 study in the European Spine Journal used multimodal imaging indicating 67.64% patients with Modic Changes had a score of 6, indicating high infection possibility, resembling infection rather than trauma suggesting the possibility of an infective cause.
A 2022 study in the European Spine Journal used multimodal imaging indicating 67.64% patients with Modic Changes had a score of 6, indicating high infection possibility, resembling infection rather than trauma suggesting the possibility of an infective cause.
A 2022 study in World Neurosurgery indicated antibiotics and bisphosphonates improved treatment in patients with Modic Changes. Patients with Modic I and disc herniation experienced poorer improvement with conservative treatment, while significant variability exists in outcomes following steroid injections.
The authors concluded, “Non-operative therapy may provide patients with MC with significant benefits. Patients may benefit from therapies not traditionally utilized for LBP such as antibiotics or bisphosphonates, but conservative therapy is not recommended for patients with concomitant MC and disc herniation.”
While percutaneous endoscopic interlaminar discectomy (PEID) is one of the main techniques with good results in treating lumbar disc herniation, a 2023 study in the Journal of Pain Research found postoperative pain and functional status of patients with type I or severe Modic changes tend to deteriorate as time goes by.
A 2023 study in The Spine Journal used a new system based on disc-endplate-bone marrow classification (DEBC). This sytem produced Type-A: Acute inflammation; Type-B: Chronic Persistence; Type-C: Latent and Type-D: Inactive. An H+ modifier was added with presence of disc herniation. Type-B was found to be the most common. The authors indicate better predictability for the need for surgical intervention and incidence of postoperative infection rate. The need for surgery was most prevalent in the DEBC with H+. They note previously undetected inflammation indicating increased deleterious activity compared to previous classification.
A 2023 study in the Journal of Pain Research found out of patients with back pain, 7.7 percent of segments displayed Modic changes, with 35.5 percent indicated as Type I, most being type II. Changes were correlated with disc protrusion, extrusion and sequestration, Schmorl’s node, and stenosis. While not associating specific types with symptoms, the authors note a destabilizing effect, recommend more aggressive anti-inflammatory treatment, and indicate they “… are a very important factor in low back pain.
A 2023 study in Infection and Drug Resistance found Modic changes as a risk factor for surgical site infection following lumbar surgery. The authors indicate, “Therefore, Modic changes are not only a manifestation of lumbar disc degeneration but also that of chronic inflammation and should hence receive added attention from clinicians.” In spinal surgery, surgical site infection is associated with prominent morbidity, health care expenses due to readmission and reoperation, as well as poor prognosis.
A 2024 study in the European Spine Journal identified specific and significant circulating blood biomarkers associated with symptomatic patients with lumbar Modic changes, regardless of disc alterations, degeneration and/or herniations/bulges. Differences in C-C Motif Chemokine Ligand 5 (CCL5) and Macrophage Migration Inhibitory Factor (MIF) protein levels were significantly noted in Modic patients compared to those without.
A 2024 study in the European Spine Journal found Modic changes may be a potential risk factor for surgical site infection after posterior lumbar spinal intervertebral fusion. Type I and grade C changes showed a greater infection rate compared with other types and grades.
A 2024 study in Orthopaedic Surgery indicates preoperative Modic change of the cervical spine was significantly associated with heterotopic ossification formation after cervical disc replacement and should be identified as a potential risk factor.
A 2024 study in Arthritis & Rheumatology found Infliximab was not more efficacious than placebo in reducing pain related disability in patients with moderate to severe chronic low back pain with Modic changes type 1 at 5 months.
A 2024 study in PeerJ notes identified as an independent risk factor for low back pain and found higher incidence of MCs post-lumbar discectomy, particularly from preoperative absence of MC.
So we have a distinct picture that I have postulated from the very beginning of this article (Published on: Jun 28, 2014): Type I Modic changes are a specific disease process associated with spinal pain and inflammation that are less responsive to treatments, associated with poor healing, recurring and long lasting disc herniations. Modic I changes represent a rapid, unstable, destructive type of spinal degeneration with a significant percentage associated with a low virulent bacterial infection.
Factors involving genetics, injury, inflammation and infection are proposed etiological factors. These processes can be closely interrelated and each might play a role in the chain of events leading to Modic Changes. Additionally, there must be consideration for the age of the patient. Obviously, Modic changes are seen with more advanced age; however, when seen in a patient in their 30’s or formative working years, and this includes high levels of disability, something should be done instead of saying nothing works and it’s all in your head. I have seen and been involved in Antibiotic therapy and diagnosis that have saved careers and a lifetime of suffering and disability.