
Understanding The Lumbar Spine & Structures Responsible For Back Pain
There are many causes of back pain, that is why it is always recommended to seek advice from your health care professional. We will discuss the lumbar spine and its relationship to common sources of low back pain.
The lowest part of the spinal column is called the lumbar spine, this is your lower back which is made up of 5 spinal bones called vertebrae. At the bottom or base of the lumbar spine is the sacrum that connects to the pelvis. Rarely, x-rays may show an extra lumbar vertebra (spinal bone) that really is one of the bones of the sacrum that did not fuse. While this can cause some issues with back pain, it is not a serious finding and poses no danger.
The arch in the small of your lower back is due to the shape of the spinal bones, which forms a backward facing “C” is called a lordotic curve. This is similar to the neck or cervical spine and opposite to the thoracic spine, which is your mid and upper back. Loss of the normal lordotic curve in the low back can be from muscle spasm or related to degeneration or posture issues.
The lower back is particularly vulnerable to stress because it connects with the pelvis. This forms your center of gravity, where much of the body motion takes place and bears a lot of weight. This combination of weight bearing with motion makes the low back at risk for too much stress from lifting, bending and twisting, as well as constant pressure from long periods of sitting and poor posture. Either from from long exposures to mild stresses or one big overload, damage can result to the structures of the lumbar spine causing pain and a decreased ability to function normally.
 Traction & Inversion
Traction & Inversion Supports & Cushions
Supports & Cushions Belts & Corsets
Belts & CorsetsLumbar Spine Structures
Spinal Bones
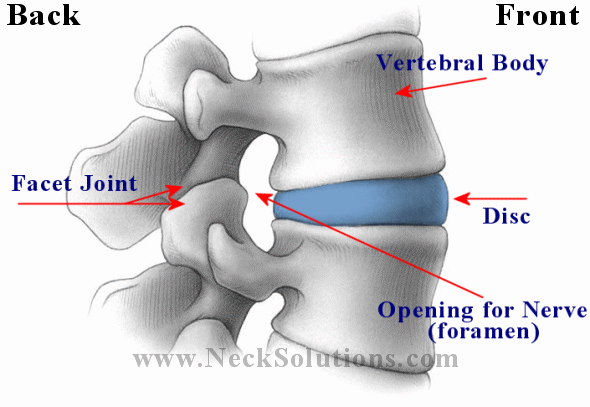
The lumbar spine is made up of bones (vertebrae) which are stacked on each other with a disc between each one which helps ease pressure as well as keeping bones at a proper distance to prevent bones touching each other and free nerves of any pressure. The bones attach to each other by ligaments and muscles are connected to the bones by tendons. Ligaments connect bones to bones; tendons connect muscles to bones. There are also tendons that fasten muscles to the vertebrae. The bones also have joints, similar in function to the elbow or knee. These are the facet joints and help the bones glide during motion. In the center of the bones, there is a opening which forms a tube for the spinal cord, and in the lumbar spine, nerves come off the spinal cord before going out through the bones. The bundle of these nerves in the lumbar spinal canal or tube are called the cauda equina, or horse tail. Nerves that come off the spinal cord have roots that exit through openings between the bones called foramina.

Spinal Discs
The discs between each bone (intervertebral discs) are round structures that function as cushioning and provide motion between the bones. A soft center portion called the nucleus and a tougher outer portion called the annulus, a ligament which helps protect the inner portion of the disc. The soft nucleus portion serves as a shock absorber and a ball bearing for motion. The nucleus contains large amounts of water and acts like a water bed.
Spinal Joints
The facet joints meet between each bone on either side, so there are 2 facet joints between each vertebra. They overlap, forming a joint between 2 bones, allowing spinal flexibility and smooth motion. They are covered with a spongy, slippery material called articular cartilage that prevents friction during gliding motion. The facet joints are surrounded by a joint capsule, which is a water tight covering of ligaments and tendons, which keep the two joints in place. The joint capsule contains fluid called synovial fluid to lubricate the joints, decreasing friction, similar to oil lubricating an engine.
Spinal Foramen
Because the foramen between each bone forms an opening for the nerve, they are called neural foramen. This is where the nerve goes through the bone to parts of your body. The part of the nerve that goes through the bone is called the nerve root. Each lumbar vertebra has 2 neural foramen, one on either side. This is the way the brain communicates to the rest of the body, through these nerves. The signals they transmit allows the body to function properly.
Spinal Cord
The spinal cord is made up of millions of nerves which go through the center tube in the bones called the spinal canal. It starts at the brain and goes to the bottom of the first lumbar spine vertebra, where it then branches into the cauda equina (bundle of nerves resembling a horses tail), before going through the neural foramen of the bones, where it forms the nerve roots. The spinal cord has a membrane over it for protection called the dura mater or dural sac, which is a water tight covering for spinal cord and nerves. The dura mater contains spinal fluid which bathes the cord and nerves. The lumbar spinal nerves go to the legs, bladder and bowel. They control muscles, organs and sending signals back to the brain, control sensations like numbness, tingling and pain.
 Massage Tools
Massage Tools Relief Supplements
Relief Supplements Topical Relievers
Topical RelieversSpinal Muscles
 Muscles along the spine are called paraspinal muscles and they provide motion as well as support for the lumbar spine. So, the joints allow flexibility, while muscles provide mobility. Close to the spine, there are many small muscles to control smaller motions between the bones, larger ones to control motion, and yet larger muscles that connect the spine to other parts of the body. A muscle, when injured is called a strain. Muscles can go into spasms. A muscle goes into spasm when it tightens up and does not relax. This is a reflex muscle contraction that is not under your control. Although painful, they can help protect discs, nerves, ligaments or other muscles of the lumbar spine. The pain of a back muscle spasm can produce a burning sensation from continuous contraction, causing narrowing of the blood vessels and the build up of lactic acid, a chemical from over-contraction of muscles, like muscle soreness from a strenuous workout. As the spasm eases, fresh supply of blood removes the lactic acid.
Muscles along the spine are called paraspinal muscles and they provide motion as well as support for the lumbar spine. So, the joints allow flexibility, while muscles provide mobility. Close to the spine, there are many small muscles to control smaller motions between the bones, larger ones to control motion, and yet larger muscles that connect the spine to other parts of the body. A muscle, when injured is called a strain. Muscles can go into spasms. A muscle goes into spasm when it tightens up and does not relax. This is a reflex muscle contraction that is not under your control. Although painful, they can help protect discs, nerves, ligaments or other muscles of the lumbar spine. The pain of a back muscle spasm can produce a burning sensation from continuous contraction, causing narrowing of the blood vessels and the build up of lactic acid, a chemical from over-contraction of muscles, like muscle soreness from a strenuous workout. As the spasm eases, fresh supply of blood removes the lactic acid.
Lumbar Spine Pain
Compression pain results from irritation or pressure on the nerves or spinal cord. In a disc herniation, the herniation can press on a nerve causing weakness of the muscles, tingling, numbness and pain from the nerve being pinched. Another type of pain involving the mechanics of the lumbar spine, like inflammation from an injured muscle, ligaments, joint or disc is called mechanical pain and hurts the more you use it. Mechanical and compressive pain from the lumbar spine can help determine what structures are involved, but it is possible to have both at the same time.
Arthritis
 Arthritis of the spine indicates joint inflammation and can produce a mechanical back pain. However, degeneration may result in bone spurs and narrowing of the disc and openings for nerves that can result in compressive pain as well. In the lumbar spine, the main cause of arthritis is a wear and tear or overuse type called osteoarthritis. It is also related to genetics and injuries, causing inflammation and destruction of the joints.
Arthritis of the spine indicates joint inflammation and can produce a mechanical back pain. However, degeneration may result in bone spurs and narrowing of the disc and openings for nerves that can result in compressive pain as well. In the lumbar spine, the main cause of arthritis is a wear and tear or overuse type called osteoarthritis. It is also related to genetics and injuries, causing inflammation and destruction of the joints.
Osteoarthritis is breakdown of the cartilage in the joint, which provides cushioning and smooth motion. The damaged cartilage is unable to heal itself, thus progressively deteriorating, decreasing flexibility and increasing the risk of further injury. Over a period of time, cartilage can completely wear away, allowing the bone surfaces to rub against each other, wearing away the joint and often forming bone spurs to try stabilizing the joints.
- One of the cardinal features of arthritis is degenerative disc disease. A 2022 article in World Neurosurgery indicates “Lumbar disc degeneration is one of the leading causes of chronic low back pain.” The progressive nature results in disc bulging and loss of water content leading to the loss of disc height.
Facet Joint Syndrome
Facet joints can be the cause of back pain. As the spine degenerates from arthritis, the facet joints often become involved. The pain from a problem with the facet joints are sometimes called facet joint syndrome. It can be caused by degeneration, arthritis or injury, which overload the joints. Because the facet joints are towards the back of the spine, pain from a facet joint syndrome may be made worse when bending backward (extension) or with twisting (rotation).
Often, overloading of the facet joints is due to disc degeneration. When the discs degenerate, the space it holds up narrows and effects the alignment of the facet joints. This places excessive loading on the joints, damaging the protective cartilage and joint fluid that lubricates the joints. Bone spurs often form around the joint and can not only affect the joint, but can narrow the neural foramen opening, causing a pinching of the nerve root. The spurs may also grow into the spinal canal called spinal stenosis and may effect the nerves or the dural covering of the spinal cord.
 New Mattresses
New Mattresses Heat Therapy
Heat Therapy Cold Therapy
Cold TherapyLumbar Radiculopathy (Pinched Nerve)
Radiculopathy is a medical term for pathology of the nerve root, often called a pinched nerve in the lumbar spine. Radiculopathy happens to a nerve that is irritated by a bone spur or herniated disc pressing or rubbing the nerve. Sometimes, when the inner part of the disc (nucleus) herniates outside the disc (annulus), called an extrusion or extruded disc, there can be a chemical reaction that causes pain and inflammation of the nerve, felt as radiculopathy.
Irritation or pressure on a nerve can cause numbness, tingling and pain in the area the nerve supplies sensation, like in pain of sciatica. So, even though the problem is in the lumbar spine, radiculopathy can make it feel like tingling in the foot. The muscles supplied by the nerve may be weak, reflexes associated with the nerve may be decreased. So, pain and other sensory location, reflexes and muscle weakness can help a doctor determine which nerve is involved from lumbar radiculopathy. Radiculopathy causes include: bone spurs, disc herniations, possibly fractures or tumors.
Sciatica
The sciatic nerve is the largest nerve in the body and is made from one or more nerves that form the sciatic nerve that runs down the leg. Sciatica is often a radiculopathy that pinches or irritates the nerve. It has a distinct name due to it being a common form of radiculopathy. It can also produce back pain in the lumbar spine at the site of irritation. So, sciatica is a term that describes the pain from the nerve. The nerve starts in the back, goes into the hip, back of the thigh, and may even go into the bottom leg and foot.
Spinal Cord Pressure
We have seen how individual nerve roots are affected by pressure and irritation — but what about the spinal cord itself? Pressure on the spinal cord typically results from a condition called stenosis. Stenosis means narrowing of an opening or tube – in this case the spinal canal.
Spinal Stenosis
Narrowing of the tube formed by holes in the bones of spine is called spinal stenosis. Stenosis means narrowing, and this can happen to any opening. When it is from the tube that the spinal cord runs through, it is often called central stenosis, as opposed to foraminal stenosis. It is often found in the lower back and can be the entire lumbar spine or just a portion or segment. The canal can be narrowed by things like degeneration, including arthritis, bone spurs and thickening of ligaments, small bones, herniated discs, infections, trauma and tumors. All of these can push into the spinal canal, making less room in the tube.
This central spinal stenosis can irritate nerves, causing pain and dysfunction. Oxygen and blood supply can also be reduced, causing numbness and pain. Additional symptoms may include pressure from the spinal cord called myelopathy. This can cause problems with walking, a heavy feeling and/or weakness in the legs, and pain during walking or standing for extended periods. The symptoms may be alleviated with rest.

Due to degenerative changes, the structures of the spine can have a pinching effect on the spinal cord. This is called pincher spinal stenosis. In the side view example above, we have a protruded disc and ossified or hardened ligament (posterior longitudinal ligament) one the left side, and a buckled ligament flavum on the right side. This can be seen in the cervical spine.
In lumbar spinal stenosis, the most common presenting symptom is called Intermittent Neurogenic Claudication (INC), also called Pseudoclaudication. This is back pain, leg pain, and weakness that significantly effects the ability to walk or ambulate. As opposed to vascular causes and conditions like diabetes, those with INC have abnormal normal pulses and vascular studies. When vascular, leg pain is more severe than back pain after walking with quick pain relief at rest.
Lumbar stenosis has no symptoms when seated and improvement of symptoms when bending forward, along with a wide based gait. Bending forward or flexion of the lumbar spine, like when using a shopping cart or bicycle, improves symptoms because extension or bending back, even straightening up, further narrows the spinal canal, thus worsening the symptoms.
 TENS Therapy
TENS Therapy Posture Braces
Posture Braces Ergonomic Aids
Ergonomic Aids- A 2021 study in the Spine Journal found that stenosis is often complicated and cannot be defined by the diagnosis alone. For those with stenosis, back pain, buttock and leg pain were associated with endplate defects, Modic changes, disc degeneration and disc height. The authors concluded that low back pain in patients with stenosis should be carefully assessed for other clinical factors and endplate defects.
- A 2023 study in The Spine Journal found lumbar spinal stenosis can also cause paraspinal muscle wasting and infiltration of these muscles in the back with fat, which can worsen stenosis because of the resultant spinal instability.
- A 2022 study in JAMA indicates approximately 103 million people worldwide and 11% of older adults in the US suffer from lumbar spinal stenosis. The authors indicate conservative first line therapy is activity modification, analgesia, and therapy, with selected patients experiencing continued activity limitation and pain may be candidates for decompressive surgery.
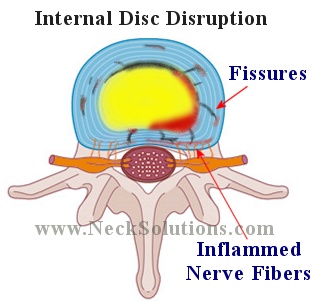
Disc Pain
Pain from the disc itself is often called discogenic pain and results from damage to the disc. Degeneration of the disc can be painful and the outer part of the disc can tear, causing painful movement of the spine located in the low back, but may also radiate into the hip or thigh.
Bulging Disc
A bulging disc is a common finding on an MRI and are not a reason to panic. They can be seen in people without any pain and can be part of a normal, age related degenerative process. Bulging discs become problematic when the bulge is enough to cause stenosis of the canal or foramen. A bulging disc, in combination with bone spurs may be enough to cause symptoms. Sometimes, an injury can cause a tear in the outer annulus of the disc, allowing a bulge of the inner nucleus to push the annulus out. This can cause discogenic as well as radiculopathy symptoms.
Herniated Disc
When the outer annulus of the disc is torn or damaged, the inner nucleus herniates from its location towards the outside of the disc. If the outer annulus of the disc tears near the side of the spinal canal, the nucleus can herniate into the spinal canal, causing pressure on the cord as well as the nerve roots. The nucleus is meant to be inside the disc, therefore, when it herniates outside the disc, a chemical reaction can cause a great deal of inflammation to the nerve, which may be very painful. Therefore, controlling inflammation is very important with the initial stages of a herniated disc in order to control pain.
Both inflammation and pressure on the nerve from a lumbar herniated disc can effect the function of the nerve, resulting in acute pain, numbness and weakness of the nerve and the structures it supplies. Herniated discs are often located in the lumbar spine due to the loads it must support. A herniated disc frequently produces sciatica, with symptoms of low back pain and tingling/numbness radiating into the back thigh, side of the leg, and even the foot. Depending on conditions, leg pain may be the primary symptom.
Because the disc is most pressurized in the morning, it is wise to wait about an hour before doing any heavy lifting to avoid the risk of disc herniation. A herniated disc does not mean surgery. Most are treated with conservative therapies and some will heal on its own. However, if the pain and function are getting worse, surgery may be indicated. Sometimes herniated discs do not heal and are complicated with Modic degenerative spinal changes, some of which are related to bacterial infections producing back pain, making them resistant to treatments and producing a long lasting back pain.
Rarely, a lumbar spine herniated disc may be large enough to place significant pressure on the spinal cord, causing a medical emergency called cauda equina syndrome. This poses the risk of paralysis of muscles controlling the bladder and bowels.
- A 2020 study in The Spine Journal found the disc absorbs loading in lateral/side bending and shear, while the facet joints and their capsules stabilize axial rotation. The anterior longitudinal ligament resists extension while ligamentum flavum and posterior longitudinal ligament stabilize flexion. While there is small variability of contribution, there are some distinct adaptations of the structures to one another regarding stabilization.
Instability
- According to a 2021 study in BMC Musculoskelet Disorders Lumbar spinal stability is the ability of the lumbar spine to tolerate displacement during normal loads and postures without generating pan. Lumbar stability is achieved through the combination of passive, active and neural control systems. When at least one of these are compromised, lumbar spine movement can become abnormal.
Patients with lumbar instability had a longer duration of symptoms and a higher frequency of pain radiation, higher disability scores, and most observed at the L4/5 level due to the orientation or inclination of the of the joints. It has been identified in up to 57% of chronic low back pain patients. It can lead to pain, functional limitations and reduced quality of life, as well as further development into surgical treatment. Prompt detection is crucial and appropriate conservative treatment, such as exercise stabilization, which focuses on deep trunk muscle training, can improve or delay the development of lumbar instability.
Lumbosacral Transitional Vertebrae
Most commonly, lumbosacral transitional vertebrae can be found in up to 30% of the population. There are a variety of anomalies that can affect the lumbar spine. Sacralization of the last lumbar vertebral body forms an articulation that produces and extra sacral segment and lumbarization of the top sacral segment produces an extra articulation of the lumbar spine, often an extra lumbar vertebra.

These conditions may demonstrate varying structural possibilities that range from an elongation of a part of the bone to complete fusion. Back pain can be associated with instability and other factors related to the psuedoarticulation or false articulation.
Correct identification is essential due to important clinical implications. Inaccurate identification may lead to surgical and procedural errors and confusing symptom correlation. The relationship between these anamolies and pain is often termed “Bertolotti Syndrome,”. Bertolotti’s syndrome was first described nearly a century ago. Symptoms can originate from the anomalous articulation, the opposite facet joint (when one sided), instability, early degeneration and nerve root compression.
- A 2021 study in the Spine Journal indicates Bertolotti syndrome to be an elusive cause of chronic low back pain. Patients can experience symptoms similar to common degenerative diseases of the spine, With a pseudoarticulation, a semi-mobile joint with cartilaginous surfaces may arise. Treatment outcomes are not well understood but can involve diagnostic as well as therapeutic injections and ultimately surgical removal of the pseudoarticulation (pseudoarthrectomy) or fusion of surrounding segments.
The authors concluded that proper and timely identification alters the clinical course of these patients as they can only be offered treatment directed towards the lumbosacral transitional vertebrae once it is identified.

- A 2019 study in the Journal of Neurosurgery concluded, “Bertolotti syndrome patients have a condition that affects them potentially more significantly than those with lumbosacral radiculopathy, and increased attention should be paid to these patients to improve their workup, diagnosis, and treatment.”
- A 2021 study in Spine found lumbosacral transitional vertebrae were associates with higher prevalence of facet degeneration, disc degeneration, disc herniation Modic changes and back pain.
- A 2022 study in European Radiology found lumbosacral transitional vertebrae have more severe disc and facet joint degeneration. The authors found increased vertebral body cross sectional area throughout the lumbar spine, which could be a contributing factor.