
Chiropractic Management Of Modic Changes
Speaking as a Chiropractor, I think many of us have had the experience of treating low back pain with little significant results. Many of us may have had the experience of being reviewed and denied care for our patients based on studies showing degeneration is as common in those without back pain as those with back pain. We frustratingly prescribe maintenance care for ongoing short term relief, however, how many of our patients have been suggested to have a psychological related condition, rather than a specific back pain condition for lack of a pain generator. We will discuss a specific pain generator that can be missed as a possible complicating factor for chiropractic management of Modic changes.

We cannot really take this to heart, as we know that central hypersensitivity does exist, inasmuch as there may have been a pain generator, but not anymore, and we know symptoms can persist on this basis, however; it does not provide good clinical reasoning for continued active care without a specific pain generator responding to specific therapeutic measures. We often are accused of perpetuating psychosocial factors by continuing care.
However, we know, as indicated in the 2014 issue of BioMed Central Psychiatry, “Pain, not chronic disease, is associated with the recurrence of depressive and anxiety disorders.” Are we doing patients a favor by saying we don’t know what it is, so we can’t get insurance to pay for any treatment? Conversely, are we doing the patient a favor with repeated adjusting and/or therapy directed to a possible infected disc? A specific disease entity? Do we even know? Do we care? We better!
The literature supporting Modic type 1 changes as a specific pain generator, indicating a particularly rapid form of symptomatic, deforming degeneration and a specific pathologic entity, is well established. Now we understand that some, about 30 to 40%, are related to infection and these modic changes may respond to antibiotics, intradiscal injections of steroids or bio-cement, various medications and even surgery.
How about Chiropractic care? Modic 1 changes related to strictly structural factors may respond to some of the previous methods, however; it would be interesting, now that DWMRI appears to distinguish between infectious and non-infectious modic changes, to follow future studies relating to structural therapies including manual treatments to support clinical reasoning for modes of therapies more commonly associated within the realm of Chiropractic. Time will tell if there is a role for chiropractic management of Modic changes, however, it is clear they are a complicating factor that should be noted.
Until then, it is difficult to formulate clinical reasoning supporting Chiropractic or Physical Therapy in the treatment of Modic type 1 associated back pain other than palliative care associated with antibiotic therapy, as in enhancing absorption of antibiotic, possibly with flexion distraction type therapy. Do we use traditional adjusting/manipulation to a Modic type 1 segment? Is there a risk of promoting microfractures or, as indicated in the 2013 edition of the Archives Of Physical Medicine And Rehabilitation, would high-velocity low-amplitude manipulation have a positive effect on the functional status of the disc by increasing height, flexion as well as related pain, thereby providing enhanced absorption of antibiotic or promoting biomechanical stability?
We know from Dr. Albert’s 2013 study that patients were allowed to continue pain medication as needed during antibiotic therapy, therefore, clinical reasoning might include palliative, biomechanical and/or enhancing therapeutic measures during antibiotic therapy, as well as biomechanical support for those who are indicated not to have infection associated Modic changes. Typically, the lumbar spine displays instability on dynamic flexion/extension radiographs, where the cervical spine may display restricted motion.
Advances in cold laser therapy technology are needed to penetrate depths necessary (7-15cm) to effect an anti-inflammatory response to Modic changes. This could be a reasonable alternative to intradiscal steroid injections for short term relief.
While epidural injections are often promoted for radicular components associated with Modic degeneration, I have found no supporting literature indicating any effectiveness for Modic type 1 changes. Well, we could say the same for Chiropractic, but that has to change. The significance of Modic 1 degeneration should necessitate us to research our role for possible effectiveness in primary or adjunct treatment.
Chiropractic Management Of Modic Changes: Reducing Inflammation
We know from an article in the 2014 Endocrine, Metabolic & Immune Disorders – Drug Targets journal that Vitamin D has antibiotic properties. It was also reviewed in a 2014 issue of Annals of the New York Academy of Sciences, where the authors indicated Vitamin D “…may be useful as an adjuvant therapy in diverse infections.”
Additionally, we know form a 2015 study in the journal Lupus that 4000IU of Vitamin D a day reduced tnf-alpha in subjects with musculoskeletal pain by over 50%. Vitamin D deficiency has been implicated in spinal stenosis, with almost 75% of patients being deficient, and direct relationship established with severity of pain, according to a study in a 2013 issue of Pain Physician.
Reducing tnf-α can be an important focus. It plays a key role in disc degeneration and Modic changes regarding levels of inflammation. A previous study in a 2000 edition of the journal Spine indicates tnf-α to be a significant inflammatory factor in nerve root pain.
Furthermore, a 2008 study in Spine acts as fertilizer for axon nerve growth into a degenerated disc, inducing disc degeneration. A 2015 PloS One study indicates tnf-α has the ability to penetrate and damage healthy discs causing damage and dynamic stiffness.
Therefore, the use of vitamin D, as related to antibacterial and a tnf-α reducing properties can be an important recommendation. Curcumin, a natural polyphenol has been used to treat inflammation. A 2015 study in European Review for Medical and Pharmacological Sciences indicates curcumin significantly lowers tnf-alpha in the lumbar disc tissue. The optimal dose is not indicated, however, results were similar for high or low dosages.
Chiropractic Management Of Modic Changes: Subjective & Objective Findings
This is an important role in documentation for chiropractic management of Modic changes, which display signs of endplate disruption, whereas typical age/genetic degeneration maintains endplate integrity. Modic changes are graded by the Nordic Modic Protocol, based on the percentage of the endplate and bone effected. MRI is the standard for discerning these changes, however, the use of high field units will show more Modic 2 than Modic 1, confounding the diagnosis. Low field units are best at determining Modic 1 changes due to the fibrovascular tissue and high water content. 3.0 Telsa units are not good for showing Modic changes.
With the advent of more high field units, many modic 1 changes will go undiagnosed, mostly noting reports of “reactive endplate changes” [Modic changes], but not type or grade. STIR sequencing can help differentiate. Schmorl’s nodes are typically seen, reflecting an intradiscal herniation that is usually painful for a few years then subsides, however, they may be directly associated with modic changes in some cases. Modic changes are closely associated with decreased disc height and disc herniation.
Differentiating Types Of Modic Changes On MRI
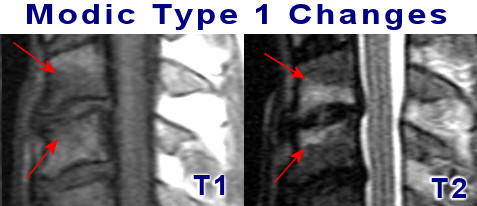
Discerning Modic changes and the type present depends on fluid signals regarding the pathological process. Type 1 is fibrovascular tissue, Type 2 is fatty degeneration and Type 3 is sclerosis or scar. This is seen as hyper or hypo-intensities; light or dark signals seen on T1, T2 and STIR sequences. There may be mixed types like 1/2 or 2/3, as well as different levels containing different types; modic changes are a dynamic disease process.

This can be a helpful tool for diagnosing type of Modic change on MRI
| Type/Sequence | T1 | T2 | STIR |
| Modic Type 1 | Dark | Light | Light |
| Modic Type 2 | Light | Light | Dark |
| Modic Type 3 | Dark | Dark | Dark |
Grading Modic Changes
The Nordic Modic Protocol has 4 grades: 1 – endplate only (A), 2 – up to 25% (B), 3 – 25-50% (C) and 4 – > 50% (D). Most are type 2, followed by type 1, then mixed, and the least prevalent are type 3. The prevalence in clinical populations is about 40%, about 6% in the general population. Typically, type 1 lasts about 3-5 years, then type 2 for about 5-7 years, however; Modic type 2 has been noted to change back to Modic type 1, so this time frame is basic and may be shorter or much longer.

We must remember the limitations regarding different types and capabilities of MRI units, however, we should be able to discern type and grade of Modic changes from MRI scanning, when reports are not clear. Noting this could be considered a complicating factor, or necessitate referral. A referral does not mean you lose the patient. There can be clear clinical reasoning for maintaining care, depending on the type of treatment the referral indicates.
Are Modic changes a complicating factor? That depends on the subjective and objective findings. Since not all changes are associated with infectious components, only ones fitting the specific criteria would be. A 2019 study in the Journal of Manipulative & Physiological Therapeutics noted no difference in outcomes for low back pain in those with Modic changes or without.
However, the subjects in the study had nonspecific back pain without disc herniation. This would not fit the criteria for a complicating factor other than possibly grade of disc degeneration. Therefore, it is important to establish the diagnosis as a direct result of Modic changes, specifically type I, through objective and subjective findings for back pain. The cervical spine seems more general with particular complications with changes at C7-T1.
There is not much data on symptoms related to cervical Modic changes, however, a A 2020 study in Neurospine examined the effects of cervical spine Modic changes on outcomes of surgical ACDF. They required larger fusions and had longer duration of symptoms pre-surgery. The authors concluded, “While MC may not affect specific outcomes following ACDF, they may indicate a more debilitating preoperative state for patients.” They noted changes at C7-T1 level displayed higher disability levels following surgery.
The odds ratio for Modic changes and back pain is 4.5 – very high. We also have some information on symptoms and findings for lower back pain.
A 2021 study in the Journal of Pain Research indicates Modic 1, severe Modic changes and multi-segmental lumbar Modic changes were significantly linked to lumbar sagittal imbalance and lumbopelvic sagittal parameters.
We know there is usually a history of chronic back pain consisting of exacerbation and remission, with risk factors being disc herniation and increased age. We note that disc herniations do not always cause pain; herniations may not impinge on a nerve root or compromise the central canal. There may be localized back pain, but typical care often resolves this.
Modic changes are often disabling and long lasting; about 80% have constant pain which varies in intensity, but is always there – most likely a result of PGP 9.5 unmyelinated nerve fiber infiltration in response to tnf-&;alpha and other inflammatory cytokines. A prevalent finding is waking with pain at night from turning in bed, which can be an indication of microfractures. Experiencing a microfracture is a very unsettling and painful experience.
The pain pattern is typically inflammatory, with pain worse in the morning, better at mid-day, bad in the afternoon, and worse at night. The pain is felt deep in the back and may radiate into one or both legs. The pain increases with activity; inflammation, microfractures and nerve fibers.
During examination of the subjects in Dr. Albert’s study, the most prevalent objective sign is pain on flexion – lumbar spine flexion. Note that patients will often use motion at the hips, hamstring and knees to compensate, however, actual lumbar motion may be severely restricted and painful. This can also accompany loss of disc height, reducing annular and intervertebral ligament tension, thus lessening lumbar spine resistance to flexion. This typically improves with usual care, however; with modic changes, this can become progressively worse.
The next most common finding is pain on springing – manual pressure or percussion on a spinous process may often localize this deep type of pain, often corresponding to specific area(s) of pain on lumbar flexion. The next most common objective sign would be pain on extension, followed by cranial compression. Centralization is not positive. Straight leg raising usually is localized to the lower back.
A 2019 literature review in The Spine Journal found Modic changes were found to be associated with neck pain and disc degeneration in the cervical spine. The authors indicated, “Patients with MCs were reported to experience more neck pain and disability”.
A 2021 study in the Journal of Orthopaedic Research indicate Modic changes and structural endplate abnormalities often manifest concomitantly in patients indicated for anterior cervical discectomy and fusion for degenerative pathology. Patients with endplate pathology, including concomitant Modic changes reported significantly higher levels of postoperative disability following anterior cervical discectomy and fusion.
What Is The Chiropractor’s Role In The Management Of Modic Changes?
Again, time will tell, however; it would not be wise for the Chiropractic profession to ignore or make light of Modic changes and the effects it has on our patient’s lives. We must provide clear clinical reasoning for therapeutic measures as well as to inform our patients of this disease, outside of the vertebral subluxation complex, and make referrals where necessary.
We need to be informed, in a non-biased manner, about antibiotics in the use of back pain and be able to answer some of the more frequently asked questions regarding Modic changes and antibiotics. Until further evidence elucidates more specific answers to the questions involving chiropractic management of Modic changes, it seems like a reasonable and necessary approach at this stage, and one that needs to be addressed now, rather than later.
While chiropractic adjustments can be used for biomechanical support in purely structural Modic changes, lack of objective improvement warrants further investigation. While treatment for infectious Modic changes include antibiotics, chiropractic management of Modic changes can include reasonable adjusting; perhaps flexion-distraction or low force structural support, the recommended initial education session for the patient and spouse, bracing, ergonomics, and therapies with a focus on reducing inflammation like deep penetrating cold laser. Targeted exercise should be avoided! Modic changes left untreated or treated improperly can lead to years of pain and disability.
A 2016 study in the Journal of Manipulative & Physiological Therapeutics concluded, “Modic positive patients reported higher levels of clinically relevant improvement 2 weeks, 3 and 6 months compared to Modic negative patients. However, at 1 year Modic I patients were significantly less likely to report ‘improvement’, suggesting they may be prone to relapse.”
A reasonable approach in chiropractic management of Modic changes is recommending an anti-inflammatory diet which includes 2 to 3 servings of fish like sardines or salmon a week. If your patient does not eat fish, supplementing with fish or krill oil is recommended. Vitamin D, as discussed above, along with anti-inflammatory herbs like turmeric and ginger. Avoid sugary and flour based foods in general. Paced general exercise – teach pacing.
Chiropractic Management Of Modic Changes, Spondylodiscitis & Osteomyelitis
While Modic changes can be due to an infection in the spine, Propionibacterium acnes and Corynebacterium propinquum, it is not generally been noted as Spondylodiscitis, although pain and findings on MRI may be similar. Studies with Diffusion Weighted MRI indicate Modic changes to be a slower process than “spondylodiscitis”, regardless of the infectious or structural cause. While it may not be incorrect to call Modic changes spodylodiscitis, the infectious nature would need to be supported via biopsy, or inferred by response to antibiotic treatment.
Typically, spondylodiscitis consist of spondylitis (inflammation in the vertebrae) & discitis (inflammation in the disk space). Modic changes may be a less virulent type of spondylodiscitis, however, spondylodiscitis is a crucial part of the differential diagnosis in low back, buttock, flank and groin pain. While risk factor for Modic changes are disc herniation and degenerative disc disease, risk factors for the more insidious spondylodiscitis are a previous spinal or genitourinary procedure, morbid obesity, diabetes, IV drug abuse, and those with depressed immune systems (eg, chemotherapy, malignancy, organ transplantation, corticosteroid use or alcohol abuse).
About 40 to 90% of spondylodiscitis is caused by Staphylococcus aureus. Escherichia coli, Proteus and Pseudomonas, are usually the cause after genitourinary procedures or infections. Pseudomonas infections are found in IV drug abusers. Species of Salmonella can cause spondylodiscitis, primarily from an intestinal source in those with sickle cell disease. Mycobacterium tuberculosis rarely infects the skeletal system, however, when it does, 50% is seen in the spine. Anaerobic bacteria can be associated after penetrating trauma or with diabetes. P. acnes and C propinquumor are anaerobic bacteria associated with the skin and gums and relate to Modic changes through a herniated disc, Schmorl’s node or direct pathway to the disc.
In discitis, WCC is normal, however the ESR is usually elevated. Without improvement in 4 weeks, blood work for inflammatory markers is a rational follow-up. When ESR and CRP are elevated with continued symptoms, MRI is usually done to rule out or confirm spondylodiscitis. This is where confusion may exist between Modic changes and spondylodiscitis. Thus, DW-MRI has been indicated to differentiate the 2 entities.
So, are Modic changes spondylodiscitis, osteomyelitis? A good case can be made technically for infectious related grades above 1, which are endplate involvement only. By adjusting infectious Modic changes, are we treating spondylodiscitis or osteomyelitis? Obviously, more research needs to be done. While further studies with antibiotics have yet to surface, we should take this matter seriously as studies have proven effective with biophosphonates, intradiscal injections, fusion, and bio-cement infiltration.
A 2019 study in Pain Research & Management found conservative treatment resulted in better outcomes for Modic I than type II after 6 months. The authors used conservative therapy consisting of prone McKenzie stretches (30 repetitions twice per day), pharmacological therapy (NSAIDs and muscle relaxants up to 4 weeks, bed rest (hard mattress for 3 months), decreased workload, whole body massage followed by a 30 minute back massage (once per week for 3 months).
It is not clear if symptom improvement was maintained beyond 6 months of therapy. It was not indicated if mechanical diagnosis was performed prior to the selection of McKenzie therapy. However, it is documented that conservative therapy for 6 months is beneficial for type I, while type II changes did not benefit from an additional 3 months. Therefore, this indicates clinical reasoning for documentation of type I lumbar Modic changes as a complicating factor with benefits extending to 6 months.
As one of the few that were certified in Modic Antibiotic Spinal Therapy (MAST) by Dr. Albert, and additionally have documented Modic 1 changes; I feel it is imperative that we are educated, can produce concise documentation to justify clinical reasoning, and develop professional relationships that clearly indicate chiropractic management of Modic changes is imperative. We owe that to the small, but significant number of our patients, and to the respect our profession deserves.
Review of Pertinent History Suggestive of Clinically Relevant Reactive Modic I Changes:
- Persistent and well localized back pain
- Exacerbation with exercise therapy
- Awakens during the night with pain
- More than 30 minutes of morning stiffness
- History suggesting disc herniation within the previous 2–3 years.
- Improved sciatica, but back pain persisted or increased
- Relevant conservative treatments without satisfactory effect
- Average pain intensity > 4/10
- MRI documented Modic change Type I or I/II mixed in the painful region.
A trial of chiropractic management is reasonable; however, with no response documented within a conservative trial period relevant to previous management(s). A consultation for consideration of antibiotic protocol (general practitioner) or other relevant medications (rheumatologist) is warranted prior to surgical consult.
A 2021 study in the European Spine Journal using metabolomics found an association between Modic changes and very low density lipoprotein (VLDL). The authors note a a metabolic etiology. According to the abstract, there was no age or related Modic typing in relation to VLDL in the population cohort, nor analysis of physiological etiology. This may well be a comorbid or associated finding that may indicate a risk factor.
Suggested Reading: New insights link low-virulent disc infections to the etiology of severe disc degeneration and Modic changes. Claus Manniche & Søren O’Neill, 18 Mar 2019.