
Piriformis Syndrome Is A Common Cause Of Sciatica Or Sciatic Nerve Entrapments Not Related To A Herniated Disc
Piriformis syndrome has many causes, but muscle spasm plays an important role in the origin of sensitization due to local injury, trauma, or strain. It is a myofascial pain disorder with deep gluteal pain that can radiate to the lower back and back of the thigh.
Like low back muscle spasm causing pain, the piriformis muscle syndrome may develop increased muscle tone as well. Unlike other back muscles, however, the piriformis muscle crosses the sciatic nerve. When this muscle goes into a state of sustained increased muscle tone, it therefore produces not only local muscle pain, but sciatica as well, amplifying its pain output much like the function of an electronic amplifier.
Successful diagnosis and sciatica treatment where disc herniations are absent is important because many people are affected. 1.5 million patients with sciatica severe enough to require MR imaging, only 200,000 prove to have a treatable herniated disc, therefore, a piriformis syndrome may be as common as herniated discs in the cause of sciatica symptoms.
The typical absence of a positive orthopedic signs during testing, the presence of sciatic or sciatica type pain not extending to the toes, and a negative MR imaging may account for the low rate of referral to neurosurgeons and orthopedic spine specialists.

The piriformis muscle syndrome can be accurately diagnosed and treated; additionally, it is the most common cause of persistent sciatica in those whom a proper diagnosis could not be established and in whom routine treatment fails.
- A 2018 clinical evidence update in the European Journal of Orthopaedic Surgery & Traumatology indicated the most common symptoms to be buttock pain, pain aggravated by sitting, external tenderness of the muscle and pain on movements that increase muscle tension, and limitation with leg raise testing.
- A 2019 study in the journal Muscle & Nerve indicates ultrasound to be a reliable technique for diagnosis of piriformis muscle syndrome. The authors indicated increases in cross sectional area of the affected muscle on both ultrasound and MRI.
- A 2018 MRI imaging study in Zhonghua Yi Xue Za Zhi found significantly higher thickness, area and volume of the pathological muscle. The authors found over 60% of patients presented with unhealthy sitting postures, which may related to pressure on the region causing symptoms and related muscle findings.
Causes Of Piriformis Syndrome
The pain can be related to the muscle itself, pressure on the sciatic nerve, hip bursitis and dysfunction of the sacroiliac joint or even facet joint syndrome. The pain is in the muscle area and can be referred to the buttock, hip and down the back of the thigh. The sciatic nerve pain can go down to the calf and into the sole of the foot. Pain can be referred to the groin and can be mistaken for a herniated disc.
The muscle can be aggravated by prolonged sitting on a hard surface, sitting or lying with the thigh or hip bent and knees spread apart, falling or getting hit in the muscle area, strain while twisting or lifting a heavy weight while standing with most or all the weight on one leg, a side impact car accident, driving for long periods of time with the foot on the accelerator or sitting on one foot. There may be pain on crossing the involved thigh over the other knee.
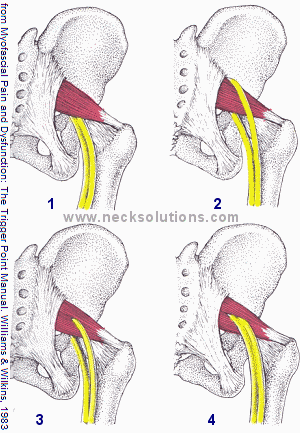
The above picture illustrates the sciatic nerve and its relationship with the piriformis. 1) The usual relationship of the nerve passing in front of the muscle. 2) The sciatic nerve looping around the muscle. 3) Part of the nerve passing through the muscle. 4) The least common is the entire nerve passing through the muscle.
- A 2020 study in Hip International used cadavers to examine the deep gluteal space and found extreme variation in the sciatic nerve origin that can contribute to piriformis syndrome.
Piriformis Syndrome Treatment
Conservative treatment that lengthens the piriformis muscle, reducing the compressive component at any given angle, should relieve the pain. However, the sciatic nerve may sustain structural damage as a result of muscle compression and may require time to heal before the symptoms are alleviated.
- A 2015 article in Current Sports Medicine Reports indicates that imaging and other diagnostic studies are usually normal and rule out other causes of sciatica. Conservative treatment includes medication and physiotherapy usually helps for most patients. For non-respondent cases, steroid and/or botox injections may be attempted. As always, guided injections using ultrasound or other imaging modalities improves accuracy of injections. If all fails and symptoms persist, tenotomy and decompression of the sciatic nerve is a surgical option.
- A 2015 study in Pain Physician showed effective relief with injections using both local anesthetic and corticosteroids injections at 3 months. This was noted for resting, in motion, at night, long duration of sitting, standing and lying.
- A 2020 report in the Journal of the American College of Emergency Physicians Open noted ultrasound guided intramuscular injection of a local anesthetic produced significant reduction of pain at 15 minutes and 48 hours after the procedure. This was done in an emergency room setting in a report of two patients.
Treatments can also be directed at other possible causes like the hip, facet joints (L5/S1, particularly with degenerative findings) and sacroiliac joints.
Stretches

Self stretch of the right piriformis muscle. The right thigh is flexed nearly 90 degrees at the hip with the right foot on the surface. Pressure is exerted downward with both hands, one on the thigh and the other on the pelvis, pulling against each other. For exercise called postisometric relaxation, attempt to press the thigh gently against a resisting left hand for a few seconds, then relax and move the thigh further down to the left to get a better stretch.
- A 2020 study in the Journal of Back and Musculoskeletal Rehabilitation found this type of progressive resisted stretching to be more effective than other types of stretching for improvement in pain, muscle length, leg raising and functional improvement.
When sleeping on the side, a pillow or body positioning pillow should be placed between the knees with support extending to the ankles. Avoid prolonged immobilization of the leg when driving a car for a long distance by stopping and walking briefly every 20 to 30 minutes. Using an active seat cushion while driving can help extend the time between breaks.
Activities which can stress the muscle like tennis, soccer, volleyball or competitive running should be reduced or eliminated for a while. Compression of the muscle may be done with a tennis ball. Lay on the back with knees bent and feet flat, place a tennis ball along the piriformis and slowly roll both legs with body to the side into the tennis ball. Make sure it is not directly on the sciatic nerve and pressure can be placed to help ease muscle spasm.
This can also be done lying on the side with the tennis ball under the muscle and the affected leg straight. Slowly pull the leg up bending at the knee, keeping the leg on the floor. You may have to pull your leg up with your hands as this can be painful. This method can help ease scar tissue stress in the muscle. Only do this a few times, slowly and breathing normally. Muscle therapy tools can help with this.
The type of stretching illustrated above can also be performed by a therapist or partner. This is a demonstration to give you a better idea of how to do it yourself or determine if you need help.
- A 2020 study in The Bone & Joint Journal uses the term deep gluteal syndrome to extends understanding of non disc related pain due to nerve entrapment beyond the traditional model of the piriformis syndrome. Deep gluteal syndrome is an increasingly recognized entity, caused by compression of the sciatic or pudendal nerve. It includes the piriformis syndrome, ischiofemoral impingement syndrome, the gemelli-obturator internus syndrome, and proximal hamstring syndrome.