
ALS Head Support – Helping Functional Head Motion & Support
A method for ALS head support is important to facilitate the negative effects of head drop syndrome that may be seen in cases of Amyotrophic Lateral Sclerosis (ALS) or motor neuron disease (MND). Although it is not the most common cause of dropped head syndrome, it can be an ominous ALS symptom that can complicate problems with breathing, swallowing and communication.
 The consequences of this symptom are significant difficulties in doing daily living activities. As a neurodegenerative disease, it affects both upper and lower motor neurons (brain and spinal cord) which may lead to progressive muscular atrophy and eventually death.
The consequences of this symptom are significant difficulties in doing daily living activities. As a neurodegenerative disease, it affects both upper and lower motor neurons (brain and spinal cord) which may lead to progressive muscular atrophy and eventually death.
As an early ALS symptom, it may originate in the medial zone of cervical cords.[1] and is unfortunately associated with poor survival time.[2] Dropped head syndrome is a vital clinical sign and often occurs as one of the early ALS symptoms within the first year or two after the onset.[3]
A head support is used in effort to maximize quality of life and minimize morbidity as a main aim in the care of amyotrophic lateral sclerosis patients. The need for specialists in multidisciplinary and palliative care throughout the course of the disease should not be minimized and can improve prognosis.[4]
A head support in ALS should be employed according to a biomechanical approach to particular neck movements, which is usually quantified by lower velocity and smoothness of motion as well as an increase in movement coupling; undesired out of plane secondary motions associated with the intended primary motion. Therefore, with side bending of the neck, there is significant unwanted rotation coupling beyond normal ranges, which makes bending the head more difficult.[5]

ALS patients experiencing neck weakness are often advised to wear a cervical orthosis like the Headmaster Collar to ease discomfort, increase ability to perform daily activities, and improve their posture. Accordingly, the collar has available supports that can be positioned selectively for increased biomechanical advantage, thus adapting to particular needs for both comfort and support. This also has the advantage of altering both number and type of supports applied, so a better level of support is offered during the disease progression.
As an ALS head support, the Headmaster Collar has been successfully used for over 30 years. Of particular note is the lightweight and breathable construction affording stable head support. The accessories like the extension pads are able to be placed together as well as individually in lateral and posterior positions offering selective fortification in support and assistance with motion.
Along with the extension pads are the anterior support to increase resistance to head drop, and the neck pad for customizable increase in posterior collar comfort and a milder level of support. The entire system permits a satisfactory range of motion where needed, flexibility of use, good appearance and comfort, with the ability to offer support and assistance for selective head motions without limiting others. Configurations range from minimally restrictive (collar only) to a more highly supportive headmaster collar setting.
Head supports are not perfect and there is always a compromise between stability and comfort when using a support for head control. Headmaster Collar, while lightweight, airy and customizable by either molding the collar by hand, using accessories or both, provides support by holding the chin, along with the chest piece as additional stabilization and assist in taking pressure from the chin.
ALS head support options consist of a drop head band systems and TLSO assisted head support systems which allow mobility and support the head using a band across the forehead as options for some. For those who use a wheelchair, the Savant Head Rest offers unparalleled support through moldable extension side pieces and a gel padded headband. It can be coupled with Axion interface for fixed placement or freedom of motion in rotation and can be fitted to a variety of headrest hardware configurations.
 |
 |
 |
Objectives For An ALS Head Support
Neck muscle weakness in patients with ALS can result in involuntary head drop or chin on chest posture. Patients with head drop frequently complain of neck pain and stiffness, embarrassment of compromised posture due to inability to make eye contact during conversation, difficulty in breathing as well as eating.
- Level of Neck Discomfort
- Communication Effectiveness
- Comfort in Social Settings
- Eating Assessment
- Hours Standing Before Discomfort
- Hours Sitting Before Discomfort
The potential benefits include possible effects on improved communication, less pain, swallowing and respiratory function efficacy. A head support should be included for consideration in the management of dropped head syndrome in patients with neck muscle weakness secondary to ALS. The devices should be measured and fitted by a health care professional and will be effective for some, but less for others.
Although Dropped Head Syndrome presents many obstacles, people can successfully control their symptoms and improve their quality of life with the correct assistive devices. The right support offers crucial relief that improves functionality and social interaction, giving individuals impacted by ALS hope and better results.
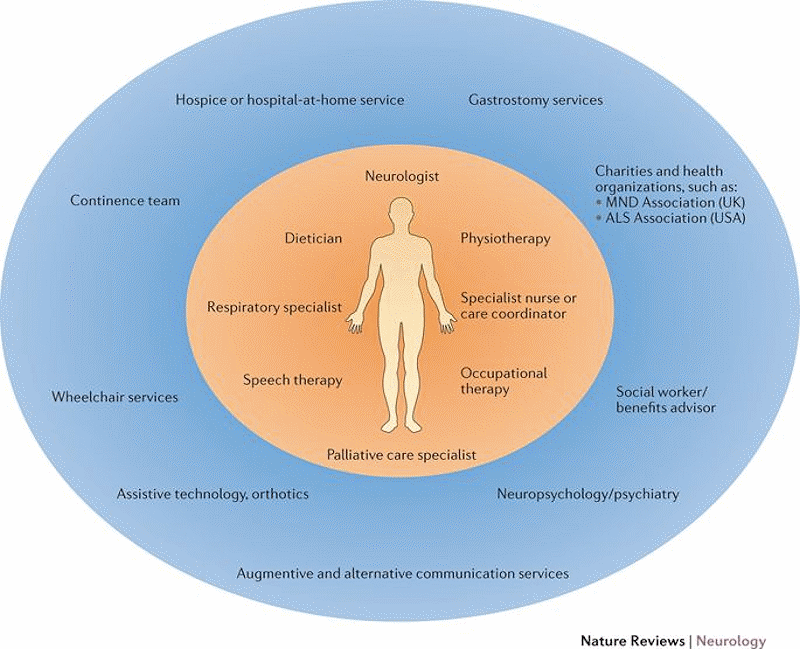
ALS Team Management
Having comprehensive management for ALS is a must. There are primary and secondary care providers that work as a team and produce amazing results. For an ALS head support, it should be prescribed by the primary provider and all measuring and fitting should be done by an Occupational Therapist. A good Physical Therapist may be of value as well for this purpose. Please click on the picture below to enlarge for the necessary components to a comprehensive team management guide.
References:
1. Neuropathology. 2019 Oct;39(5):374-377
2. Nature Reviews Neurology. 2016 Sep;12(9):526-38
3. Journal of Neurology, Neurosurgery, and Psychiatry. 2003 May;74(5):683-6
4. Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration. 2013 Jan;14(1):13-9.
5. PLoS One. 2017 Jan 9;12(1):e0169019