Cervical Radiculopathy May Cause Pain In The Neck & Arm Symptoms
Cervical radiculopathy gets its name from the neck (cervical) and compression of the root of a nerve (radiculopathy). This is caused by a disc herniation and/or the formation of bone spurs resulting from disc degeneration or cervical spondylosis.
As a nerve is pinched (compression or impingement) from these disease processes, it can produce pain directly in the neck along with radiating pain, numbness or tingling into the arm and even the hand. The numbness/tingling are called sensory deficits/disturbances or paraesthesia. Another symptom caused by cervical radiculopathy is when muscles are affected due to the nerve compression and this can cause the muscles to not function correctly, leading to weakness or loss of control of motion or strength called motor disturbances/deficits.
According to a 2020 study in the journal Physiotherapy common indications in the presenting history were arm pain worse than neck pain, provocation of symptoms when ironing, and reduction of symptoms by walking with your hand in your pocket. No complaints of paraesthesia and/or numbness decreased the likelihood of a positive diagnosis.
A 2022 study in Musculoskeletal Science and Practice indicates arm pain worse than neck pain, paraesthesia or weakness and/or numbness and/or altered reflex; MRI confirmed compression consistent with clinical findings.
Causes
As stated, radiculopathy often causes neck pain as well as radiation of this pain and/or numbness/tingling into the arm and/or hand. This occurs following the path of a nerve root (part of the nerve that is being pinched). The pain of radiculopathy can go beyond the neck (radiating) into the shoulder, arm and hand affecting muscle function and/or numbness/tingling (motor and/or sensory disturbance).
Causes of cervical radiculopathy are usually due to disc herniation, cervical spondylosis (degenerative changes), which lead to a closing or narrowing of the space which the nerve will exit the cervical spine and this narrowing of the space is called “foraminal encroachment”, leading to compression or “pinching” along with resulting irritation and inflammation of the nerve.
Therefore, foramina are the openings for the nerve and these openings can be narrowed or encroached upon by the means described above. Foraminal encroachment of the spinal nerve from degenerative changes in the uncovertebral (in the body of the vertebra) and zygapophyseal (in the back of the vertebra) joints, as well as disc herniation, where the inner, soft part of the disc pushes outside and presses against the nerve, are the two most common causes regarding cervical radiculopathy.
There are specific levels where the nerve is being pinched and this can be used to determine which disc is causing the problem. The fifth cervical nerve root comes through the disc space between the disc that sits in between the fourth and fifth cervical bones (vertebrae), so a disc herniation at C4/5 will cause radiculopathy of the fifth nerve root (C5 nerve root). Similarly, a disc herniation at the C5/6 level will lead to C6 nerve pinching or radiculopathy. The cervical spine consists of 7 bones or vertebrae along with 8 nerves or nerve roots.
Cervical radiculopathy is a neurologic condition characterized by dysfunction of a cervical spinal nerve, the roots of the nerve, or both. It usually presents with pain in the neck and one arm, with a combination of sensory loss, loss of motor function, or reflex changes in the affected nerve-root distribution.
The most common cause (in 70 to 75 percent of cases) is foraminal encroachment of the spinal nerve due to a combination of factors, including decreased disc height and degenerative changes of the uncovertebral joints anteriorly (front) and zygapophyseal joints posteriorly (back) as we have discussed with degenerative changes and cervical spondylosis. This condition also is seen in the lower back, however, herniation of the nucleus pulposus of the disc is responsible for only 20 to 25 percent of cases for the neck. Other causes, including tumors of the spine and spinal infections, which are infrequent.
There are no universally accepted criteria for the diagnosis of cervical radiculopathy. In most cases, the patient’s history and physical examination are sufficient to make the diagnosis. Typically, patients present with severe neck and arm pain. Although the sensory symptoms or paresthesias (including burning, tingling, or both) typically follow a dermatomal distribution as seen in the diagram, the pain is more commonly referred in a myotomal pattern. For example, radicular pain from C7 is usually perceived deeply through the shoulder girdle with extension to the arm and forearm, whereas numbness and paresthesias are more commonly restricted to the central portion of the hand, the third digit, and occasionally the forearm.
Weakness of the arm or hand is reported less frequently. Holding the affected arm on top of the head or moving the head to look down and away from the symptomatic side often improves the pain, whereas rotation of the head or bending it toward the symptomatic side increases the pain.
When the nerve root is pinched or has compression on it from a herniated disc, it is usually called a “soft disc herniation” due to the nature of the material pushing outside the disc, while compressing of a nerve by degenerative changes which result in excessive bone growth (hypertrophy), it is called a “hard disc” pathology, again due to the nature of the material that is causing the nerve to be compressed. In this case it is not really the disc, but the formation of bone in the joints, however, it is often called a “hard disc”. Regardless of the cause, soft or hard disc, it produces inflammation (swelling or edema) and blood vessel formation which all factor into the developing radicular (nerve root) pain.
Pain due to soft disc type herniation usually have an acute/recent incident, which may or may not present with radiation of pain/numbness/tingling in the arm/hand. Chronic (long lasting), bilateral (both sides) neck as well as radiation of pain in the arm/hand is most often caused as a result from spondylosis degeneration related to different causes, including degenerative disease of the disc as well as other neck joints.
So, chronic neck pain in association with cervical spondylosis is usually bilateral (both sides), where the neck pain of cervical radiculopathy is usually unilateral (one sided). The radiating pain will depend on which nerve is compressed, however, it is not always clear because there can be overlapping of the areas, confusing the clinical picture. A lack of pain that radiated into the arm/hand doesn’t mean there is no compression of the nerve root.
It is possible that pain is confined only to the shoulder area, and this would have to be checked to make sure there are no problems directly with the shoulder. Especially with C5 and to a lesser extent C6, which can mimic rotator cuff problems. Likewise; rotator cuff pain, especially the supraspinatus, can mimic neck pain, so it is important in differential diagnosis. Click on the picture for a more detailed view.
It is also possible that numbness/tingling (sensory) or muscle weakness (motor) dysfunctioning may occur with no major pain findings. The symptoms frequently can be worsened with neck movements such as backward bending (extension) while at the same time turning (rotation).
This motion will cause a decrease in size regarding the opening for the nerve root (neural foramen) is called “Spurling’s Test”. The doctor may press downward on the head to further compress the nerve. This is a maneuver that a doctor would perform in attempts to diagnose cervical radiculopathy. Another test is placing the affected arm up and above the head, which may open the space where the nerve exits (decompress) and provide relief of pain or other symptoms, and this is called “Shoulder Abduction Test”.
Findings on physical examination vary depending on the level of radiculopathy and on whether there is myelopathy. In most cases, the nerve root that is most frequently affected is the C7, followed by the C6. There is sometimes confusion between C4 Radiculopathy and mechanical neck pain.
A 2021 study in Medicine found that larger pain extent is associated is associated with higher headache, neck and arm pain intensity, and disability in patients with cervical radiculopathy.
A 2021 study in Journal of Orthopaedic Science found that the width of the intervertebral foramen where the nerve exits (developmental factor) and the formation of osteophytes (arthritic/spondylotic factor) were related to the onset of radiculopathy in those undergoing surgery.
A 2022 study in the Global Spine Journal indicates conservative treatment (including exercise therapy, cervical traction, transcutaneous electrical nerve stimulation, pain management education, and cervical collar) for 3 months is beneficial in the long term and avoids the risks of surgery.
Response to treatment varies depending on factors involved. Improvement should be noted within 4 to 6 weeks and significant improvement in pain and disability should occur within 4 to 6 months. Some may take 2 to 3 years to fully recover. The natural history is often favorable and conservative treatment is considered as the initial treatment of choice for cases without debilitating pain or progressive neurologic deficit.
Collars
When neck pain is significant due to radiculopathy, a brief period of immobility can help relieve the pain due to inflammation. This is often accomplished by using a neck collar. The collar should not be too rigid, nor too soft. Some have advocated the use of short-term immobilization with either hard or a soft cervical collars (either continuously or only at night) to aid in pain control. Use of a special neck pillows during sleep has also been recommended.
Traction
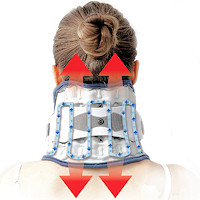
Neck traction devices devices can provide relief of radiculopathy pain by separating the vertebral bones, thus opening the space that the nerve is being compressed, offering decompression. Neck traction consists of administering a distracting force to the neck in order to separate the cervical segments and relieve compression of nerve roots by intervertebral discs. Various techniques and durations – minutes vs. up to an hour have been recommended. Recent advances in traction have made this form of treatment less expensive, easier, more comfortable and portable.
A 2021 study in PLoS One found improvement in disability, type and intensity of pain and reduced medication intake with an intensive five day traction protocol, twice a day for 30 minutes for patients suffering from cervical radiculopathy. The stress a more intensive protocol can speed recovery time, reduce sick leave and associated costs.
Medications
There is a use for neck pain medications, especially early when there is inflammation. Anti-inflammatory medications are useful for similar conditions in the lower back, therefore, an initial prescription of non-steroid or steroid medication for the neck pain as well as the radiation of pain into the arm/hand can be quite effective. There may also be a beneficial response to analgesic medications, muscle relaxers, as well as anti-depressants or anti-convulsants. Cervical radiculopathy may also respond to opioid medications for nerve pain up to 8 weeks in duration. There is not enough research to support these medications greater than 2 months.
Muscle relaxers may relieve neck pain due to spasm or an increase of tensioning of tendons, where muscles attach to bones. For long lasting or chronic nerve pain, medications can be beneficial for those who do not undergo or continue to have pain after surgical procedures. Some anti-depressants offer a fair amount of pain relief for those suffering chronic nerve (neuropathic) pain. Tramadol may also offer relief regarding this chronic nerve pain. Oral Steroids like medrol dose pack, may not have an effect on the overall course of radiculopathy, they can provide significant relief when used early in the inflammatory stage of the disease. Due to complications, long-term steroid use is not warranted and the effectiveness can decrease with subsequent use.
A 2019 study in the Journal of Pain Research found that pregabalin (Lyrica) improved pain and related sleep disturbance in patients with chronic cervical radiculopathy with pain radiating into the upper limb.
The study showed pregabalin (150–600 mg/day) for 8 weeks was more effective than other pain medications for neuropathic (nerve) pain. Oral administration is recommended at a dose starting at 75 mg twice daily (maximum 150 mg/day), then gradually increasing to 150 mg twice daily (maximum 300 mg/day) over 1 week.
Therapy
Gradual progression of physical therapy may help with restoration of motion as well as improving neck muscle strength. During the initial 6 weeks, mild motion along with stretching type exercising with massage therapy and therapeutic agents like moist heat, ice applications, ultrasound and electrical stimulation are often employed. With improvement in pain levels, gradually implemented strength exercises can be started, progressing to more active motion and resistance exercises.
A 2022 study in BMC Musculoskeletal Disorders indicates awkward posture or improper movement patterns of the cervical spine may reduce the area of the nerve opening and cause neck pain and nerve pinching. A therapeutic exercise program showed nerve opening generally increases in cervical flexion, retraction, and side bending away from the affected side.
Manipulation can also be helpful. This requires care in selection of technique, however, carefully implemented adjustments can help remove pressure on the nerve root and assist in healing, especially in the latter stages where residual affects from healing like scar tissue can limit motion and cause ongoing pain. Initially, chiropractic techniques like flexion/distraction manipulation provides careful and controlled manually applied traction using special tables. This is usually employed in conjunction with therapeutic agents described previously.
Changes in the physical characteristics of neck muscles result in indicate behavior and function changes. Fear of movement due to pain leads to a decrease in related movement. Avoidance of motion causes muscle atrophy, which can lead to more pain. Early treatment is crucial and after reduction of radicular or nerve pain, a rehabilitation program focused on strengthening is important for resolution and avoiding chronic issues.
A 2019 study in Medicine (Baltimore) found that patients with chronic cervical radiculopathy suffered significant atrophy of the deep multifidus muscles, especially at the C5/C6 level on the same side of the nerve involvement compared to the opposite side. The multifidus forms the deepest layer of the neck extensor muscle group and are important postural stabilizers.
Injections
Spinal injections of steroids are often utilized for pain control. These injections need to be administered via radiographic guiding for CT/MRI confirmed radiculopathy. The injections, sometimes called nerve blocks, directly surround the nerve root with steroid medication. It is possible to obtain pain relief within fourteen days and at 6 months following a routine of injections. It is possible that these nerve block steroid injections can reduce nerve pain and decrease the necessity for surgery. It is also possible that injections may fail to produce any results. Side effects associated with injections are not common, with minor complications in about 1.5% and a major complications less that 1%. Major complications, although rare, can be very problematic like damage to the spinal cord or possibly the brain-stem. Steroid injections can have a short term, improvement in the symptoms associated with cervical radiculopathy.
Surgery
About 33% of cervical radiculopathy sufferers who undergo treatment without surgery will experience ongoing symptoms. A basic rule is those who are not afforded pain relief within 6 weeks of conservative therapy and continue to have decreasing nerve function along with any signs of myelopathy or instability, require surgical consultation.
According to a 2021 report in the British Journal of Hospital Medicine a majority of patients improve over time with conservative management and surgery is indicated in those with significant weakness, debilitating pain, myelopathy, progressive worsening of symptoms, or instability. Surgical technique advancements provide a range of options that should be carefully considered for each individual patient.
A 2021 study in the Global Spine Journal found cervical spine endoscopic discectomy and decompression for radiculopathy due to disc degeneration had a higher success rate and lower complication rate with the posterior approach than with the anterior approach.
A 2022 study in Physical Therapy indicates conservative management of cervical radiculopathy is a first treatment option because the risk/benefit for surgery is less favorable. Initially, patient education, specific (nerve opening) exercises, spinal manipulation, and sustained pain relieving positions. In later stages, the focus should shift to include aerobic exercise, focused strength training, postural education and work related ergonomic interventions.
What Is Best Pillow For Cervical Radiculopathy?
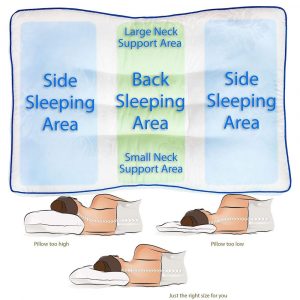
There is no “cervical radiculopathy pillow”, however, a pillow should be able to match your symptoms. With radiculopathy, certain postures will aggravate the pain, while others will help alleviate it. If your pain is worse when extending the head back – looking up, then you may want a pillow that is higher when sleeping on your back. This will maintain the head in flexion (bent forward). This should not be excessive, however, you would not want a pillow that arches the head back if this increases pain. In this case, the best pillow for would be one size larger than usual. While using 2 pillows is not recommended, you could use a small one under the pillow, or a folded towel to get more height.
The Therapeutic pillow is the most stable and, when measured and chosen according to your specific parameters, will keep you in the most natural or neutral position in both side and back sleeping positions. Reducing nerve and muscle tension while sleeping can help with healing. It is the perfect posture pillow. Being a functional pillow, it is only surpassed in comfort by the Latex Orthopedic Pillow.
The Neck Pain Pillow maintains the ergonomic advantage of allowing more room for the shoulders in side sleeping, an important factor in reducing tension and inflammation. This pillow has the advantage of allowing one side to be adjusted higher than the other. Most cases of radiculopathy will exhibit relief when bending the head away from the affected side. This can open the passage for the nerve and ease the pain. It may be the head will offer relief when bending into the affected side. Regardless, adjusting the pillow to the side that matches relief can allow for more relief when side sleeping, the most common position.
Alternatively, you can achieve a custom support with an adjustable memory foam pillow. Most pillows with adjustable fill do not contain enough foam, which causes too much effort when changing positions. This one is an exception, however, you still need to adjust the pillow every time you change positions. For some it is not a problem, while others have a difficult time. A popularly advertised pillow uses a foam fill that you adjust, however, it is a single fill for everyone. Being a professional, I get offered the professional version, which has different levels of fill depending on your preference or size, so having enough fill is very important and this one covers everyone.
Often, pain is made worse when bending the head to one side. This would affect side sleeping, and differently on each side. If the pain is worse when bending the head to the right, you need a pillow that is high enough to keep the head from tilting down to the right when side sleeping. Similarly, the pillow should be lower when sleeping on the left side. Again, a towel can be folded and placed under the pillow to achieve the best height or the Neck Pain Pillow allows adjustment of left and right sides.
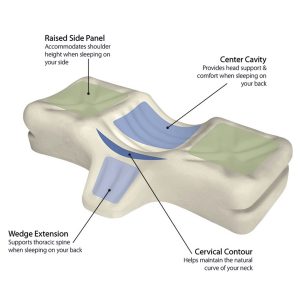
Some individuals have problems with the head turning left or right when back sleeping. This can be minimized by using a three section orthopedic cervical pillow, with it’s raised sides that help to restrict head turning while back sleeping. This can help with relief of arm pain or numbness during the night and when waking up in the morning.
So, the best pillow for cervical radiculopathy will be based on which postures aggravate and relieve the pain. By experimenting; if your radiculopathy is eased by raising your arm and placing it on your head, you may find relief by sleeping with the arm raised under the pillow. This is a clue you need higher support on that side as it will help to raise the pillow on that side or alleviate the nerve tension due to elevation of the arm. Some find the shoulder pillow offers the best solution. By using some of these suggestions, you should be able to choose a pillow, or make yours the most effective pillow.
Cervical Radiculopathy Conclusion
Combined neck and arm pain is much more disabling than either symptom alone. It is a prevalent disorder and ranks fourth in the burden of disease within the United States according to state of US health, 1990-2010 published in JAMA 2013. Younger patients (younger than 40 or 40-60) are more affected by these symptoms than patients older than 60 years. In addition, as symptom duration increases, a negative impact on mental health is observed. Patients with a significant component of neck pain in conjunction with cervical radiculopathy should be considered the most affected of all patients with cervical spondylosis.
Given the evidence that the treatment methods at the disposal of physicians are effective, prompt treatment of these patients may help avoid the harmful effects of chronic symptoms on mental functioning, especially among younger patients who were found to be more impacted by the symptoms. There is a positive correlation between intensity of neck pain and difficulty during work, leisure time, and sleep.
Stephen Ornstein, D.C. has treated thousands of neck, shoulder and back conditions since graduating Sherman Chiropractic College in 1987 and during his involvement in Martial Arts. He holds certifications as a Peer Review Consultant from New York Chiropractic College, Physiological Therapeutics from National Chiropractic College, Modic Antibiotic Spinal Therapy from Dr. Hanne Albert, PT., MPH., Ph.D., Myofascial Release Techniques from Logan Chiropractic College, and learned Active Release Technique from the founder, P. Michael Leahy, DC, ART, CCSP.

 Neck Traction Devices
Neck Traction Devices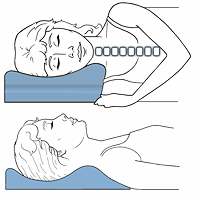 Cervical Pillows
Cervical Pillows Neck Support Collars
Neck Support Collars
 Muscle Therapy Tools
Muscle Therapy Tools Head Supports
Head Supports Topical Pain Relievers
Topical Pain Relievers Cervical radiculopathy is a neurologic condition characterized by dysfunction of a cervical spinal nerve, the roots of the nerve, or both. It usually presents with pain in the neck and one arm, with a combination of sensory loss, loss of motor function, or reflex changes in the affected nerve-root distribution.
Cervical radiculopathy is a neurologic condition characterized by dysfunction of a cervical spinal nerve, the roots of the nerve, or both. It usually presents with pain in the neck and one arm, with a combination of sensory loss, loss of motor function, or reflex changes in the affected nerve-root distribution.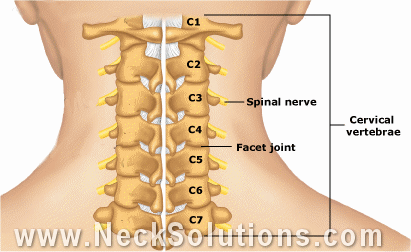
 Special Pillows
Special Pillows Heat Therapy
Heat Therapy Cold Therapy
Cold Therapy





 TENS Therapy
TENS Therapy Posture Braces
Posture Braces Neck Stabilization
Neck Stabilization Ergonomic Aids
Ergonomic Aids New Mattresses
New Mattresses Relief Supplements
Relief Supplements